
Abstract
Background
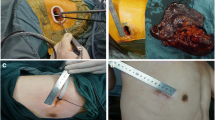
Minimally invasive surgery is considered the gold standard approach for early stage lung cancer. Techniques range from a standard three-port approach to uniportal lobectomies, with no technique emerging as superior thus far. We retrospectively compared the pain outcomes of a standard approach using a utility incision with a totally thoracoscopic technique.
Methods
Between January 2015 and December 2019, 168 patients received a VATS lobectomy in our centers. Two groups were created, Group A (82 patients, totally thoracoscopic approach) and Group B (86 patients, standard approach with utility incision). Perioperative outcomes, such as operative time, complications, length of stay, perioperative and chronic pain using visual analog scale (VAS), and rescue doses of painkillers were examined. A one-way analysis of covariance (ANCOVA) was conducted to investigate the impact of surgical time and days of drainage on VAS score.
Results
Pain was less on postoperative day (POD) 1 and 2 (p = 0.025 and p = 0.020, respectively) in Group A. No differences were found in the baseline and perioperative characteristics of the two groups, in the mean VAS score at 1 month (p = 0.429), 1 year (p = 0.561), doses of NSAIDs (p = 0.609), and chronic pain (3vs7 patients, p = 0.220). The ANCOVA test showed no significant effect of surgical time and days of drainage on VAS score (p > 0.05).
Conclusions
In our experience, a totally thoracoscopic approach may improve acute postoperative pain without compromising the oncological results of the procedure and the safety of the patients.




Similar content being viewed by others


References
Ettinger DS, Wood DE, Aisner DL, et al. Non-small cell lung cancer, version 5.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2017;15:504–35.
McKenna RJ, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: experience with 1100 cases. Ann Thorac Surg. 2006;81(2):421–5 (discussion 425-6).
Roviaro G, Varoli F, Rebuffat C, et al. Major pulmonary resections: pneumonectomies and lobectomies. Ann Thorac Surg. 1993;56(3):779–83.
Peng Z, Li H, Zhang C, et al. A retrospective study of chronic post-surgical pain following thoracic surgery: prevalence, risk factors, incidence of neuropathic component, and impact on qualify of life. PLoS ONE. 2014;9(2):e90014.
Wildgaard K, Ravn J, Nikolajsen L, et al. Consequences of persistent pain after lung cancer surgery: a nationwide questionnaire study. Acta Anaesthesiol Scand. 2011;55(1):60–8.
Taioli E, Lee DS, Lesser M, et al. Long-term survival in video-assisted thoracoscopic lobectomy vs open lobectomy in lung-cancer patients: a meta-analysis. Eur J Cardiothorac Surg. 2013;44(4):591–7.
Hernandez-Vaquero D, Vigil-Escalera C, Pérez-Méndez I, et al. Survival after thoracoscopic surgery or open lobectomy: systematic review and meta-analysis. Ann Thorac Surg. 2021;111(1):302–13.
Dolci G, Campisi A, Giunta D, et al. Video-assisted thoracoscopic surgery lobectomy using “the caudal approach”: results and evolution. J Vis Surg. 2017;14(3):187.
Bin Yameen TA, Gupta V, Behzadi A. Uniportal versus multiportal video-assisted thoracoscopic surgery in the treatment of lung cancer: a Canadian single-centre retrospective study. Can J Surg. 2019;62(6):468–74.
Balderson SS, D’Amico TA. Thoracoscopic lobectomy for the management of non-small cell lung cancer. Curr Oncol Rep. 2008;10(4):283–6.
Fournel L, Zaimi R, Grigoroiu M, Stern JB, Gossot D. Totally thoracoscopic major pulmonary resections: an analysis of perioperative complications. Ann Thorac Surg. 2014;97(2):419–24.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Maguire MF, Ravenscroft A, Beggs D, et al. A questionnaire study investigating the prevalence of the neuropathic component of chronic pain after thoracic surgery. Eur J Cardiothorac Surg. 2006;29:800–5.
Merskey H, Bogduk H. Classification of chronic pain. In: Merskey H, Bogduk H, editors. Descriptions of chronic pain syndromes and definitions of pain terms. 2nd ed. Seattle, WA: IASP Press; 1994. p. 143–4.
Vannucci F, Gonzalez-Rivas D. Is VATS lobectomy standard of care for operable non-small cell lung cancer? Lung Cancer. 2016;100:114–9.
Bendixen M, Jørgensen OD, Kronborg C, et al. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016;17(6):836–44.
Tosi D, Nosotti M, Bonitta G, Italian VATS Group, et al. Uniportal and three-portal video-assisted thoracic surgery lobectomy: analysis of the Italian video-assisted thoracic surgery group database. Interact Cardiovasc Thorac Surg. 2019;29(5):714–21. https://doi.org/10.1093/icvts/ivz153 (Erratum in: Interact Cardiovasc Thorac Surg. 2019 Nov 1;29(5):821).
Ko HJ, Chiang XH, Yang SM, Yang MC. Needlescopic-assisted thoracoscopic pulmonary anatomical lobectomy and segmentectomy for lung cancer: a bridge between multiportal and uniportal thoracoscopic surgery. Surg Today. 2019;49(1):49–55.
Dunning J, Elsaegh M, Nardini M, et al. Microlobectomy: a novel form of endoscopic lobectomy. Innovations (Phila). 2017;12(4):247–53.
Lutz JA, Seguin-Givelet A, Grigoroiu M, et al. Oncological results of full thoracoscopic major pulmonary resections for clinical stage I non-small-cell lung cancer. Eur J Cardiothorac Surg. 2019;55:263–70.
Alzahrani T. Pain relief following thoracic surgical procedures: a literature review of the uncommon techniques. Saudi J Anaesth. 2017;11(3):327–31.
Dell’Amore A, Campisi A, Giunta D, et al. The influence of the trocar choice on post-operative acute pain after thoracoscopy. J Vis Surg. 2018;4:104.
Fournel L, Zaimi R, Grigoroiu M, et al. Totally thoracoscopic major pulmonary resections: an analysis of perioperative complications. Ann Thorac Surg. 2014;97(2):419–24.
Funding
No funding used.
Author information
Authors and Affiliations
Contributions
Conceptualization—AC, MS, and FS. Data curation—AC, MT, and JN. Formal analysis—AC, APC, and JN. Funding acquisition—None. Investigation—AC and FD. Methodology—AC, GG, DA, and FD. Project administration—MS and FS. Resources—none. Softwares—AC. Supervision—MS and FS. Validation—AC and APC. Visualization—AC. Writing—original draft—AC and APC. Writing—review & editing—MS and FS.
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest to declare.
Ethical approval
The study was approved by the institutional review board of University of Bologna (the ID approval number was not produced) and written informed consent was obtained from all patients. All figures and tables are original and have not been published before.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Campisi, A., Ciarrocchi, A.P., Grani, G. et al. Totally thoracoscopic versus standard VATS lobectomies: perioperative differences. Gen Thorac Cardiovasc Surg 70, 642–650 (2022). https://doi.org/10.1007/s11748-022-01787-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-022-01787-6