Abstract
Objective
This study was conducted to evaluate the risk of recurrence possibly caused by preoperative bronchoscopic cancer confirmation in stage1A non-small cell lung cancer.
Methods
One hundred and seventy-nine cases of peripheral non-small cell lung cancer (including 151 adenocarcinoma) with no more than 3 cm in their tumor longer diameter were selected. All patients underwent preoperative diagnostic bronchoscopy followed by lobectomy, and were demonstrated to have pathologically free of lymph node involvement and pleural involvement. Radiological and pathological low-grade adenocarcinomas were excluded. Of 179 cases, 95 were confirmed lung cancer by bronchoscope (Group 1) and rest 84 had failed cancer confirmation by bronchoscope before surgery (Group 2). Forty-eight pairs for non-small cell lung cancer and 41 pairs for adenocarcinoma were identified from each group by propensity caliper matching. Kaplan–Meier method and log-rank test were performed on matched groups, and Cox proportional hazard model analysis was performed on whole matched cases.
Results
Log-rank test revealed no significant inferiority of recurrence-free survival of Group 1 in both all-NSCLC and adenocarcinoma subset. Cox proportional hazard model analysis also revealed that the ‘presence of preoperative bronchoscopic cancer confirmation’ dose not increase risk of recurrence in both NSCLC and adenocarcinoma subset.
Conclusions
It is unlikely that preoperative bronchoscopic cancer confirmation would increase recurrence risk in stage1A non-small cell lung cancer; however, a future prospective study with larger cohorts would be warranted to validate the results.
Similar content being viewed by others


Introduction
According to the fact sheet of World Health Organization and Japanese cancer information service, lung cancer is the most common cause of cancer death worldwide and in Japan, accounting for 1690 thousands and 74 thousands deaths in 2015, respectively. Lung cancer morbidity has been also increasing, though its survival rate remains still in the third lowest following bile duct cancer and pancreas cancer with a 5-year-survival of 28% in Japan.
To improve lung cancer survival, early detection and diagnosis followed by surgical resection for small peripheral lung cancers have been practiced. Furthermore, with tremendous innovations in the field of small-sized peripheral lung cancer diagnosis such as fiber optic bronchoscope with endobronchial ultrasonography-guide sheath [1] and bronchial navigation systems with ultra-thin bronchoscope [2, 3], more and more patients have come to have a confirmation of cancer diagnosis at the time of surgery.
In 2005, just around the same time to those innovations of diagnostic bronchoscope, Nakajima et al. raised the issue that preoperative transbronchial biopsy (TBB) might be a risk for recurrence in resected stage 1 lung cancer [4]. It was just the same issue that had been provoked against preoperative percutaneous transpleural needle biopsy [5, 6].
No other research have validated or even countered their result ever since; however, we always have had such threats of cancer spreading by laceration of intratumoral vessels and lympatics, or by direct spreading via airways due to preoperative bronchoscope. Thus, we challenged this study to validate the hypothesis that ‘cancer confirmation by bronchoscope’ would increase the recurrence risks in resectable NSCLC patients.
Subjects
One hundred and seventy-nine completely resected peripheral NSCLC patients (151 adenocarcinoma and 28 non-adenocarcinoma) were selected from consecutive operated cases from 1 January 2005 to 31 May 2015 in Miyagi Cancer Center, North-East region of Japan. An approval of institutional review board was obtained.
Inclusion criteria were as follows; tumor is located outer half of the lung periphery on high-resolution computed tomography (HRCT); tumor longer diameter measured on HRCT was no more than 3.0 cm (pathological diameter was also defined as no more than 3.0 cm); solid portion diameter on HRCT was no less than 0.5 cm; lobectomy and at least n2 level extent of lymph node dissection (either systematic or selective) was completed; and open thoracotomy was performed.
The reason that the tumor size had been limited to 3.0 cm (cT1a/pT1a) was that; if tumors, which were larger than 3.1 cm were included, biological strength of malignancy seemed to overwhelm possible iatrogenic effect on recurrence rate which had been observed in the previous report [4]. Similarly, to eliminate biological malignant factor as far as possible, pathological documentation for no nodal involvement, no pleural involvement and no pulmonary metastasis were completely conditioned. Observation period of censored cases was limited to at least 2 years and no more than 5 years. Upper limitation of observation period was arranged, because recurrence more than 5 years after surgery would not be fully distinguished from second lung cancer.
Exclusion criteria were as follows; multiple lung cancers; pathological low-grade adenocarcinoma (i.e., adenocarcinoma in situ and minimally invasive adenocarcinoma); cases whose diagnoses were confirmed by pre and intraoperative transpleural needle samplings; cases with complete video-assisted thoracoscopic surgery; cases with wedge resection, segmentectomy, pneumonectomy or bi-lobectomy; cases with pleural dissemination or malignant pleural effusion; and cases with intraoperative pleural lavage cytology positive for cancer cells. All those exclusion criteria were used to unify the patients’ background and to eliminate inherent biases.
Method
All selected cases were assigned to two groups by their status of having or not having bronchoscopic cancer confirmation at surgery; Group 1, preoperative diagnoses were confirmed by bronchoscopic procedures [brushing cytology positive, or ‘carcinoma’ by transbronchial biopsy (TBB)]; and Group 2, cases with negative result of preoperative bronchoscope.
Clinical information of all patients was collected from medical records: age, gender, tumor larger diameter and solid portion diameter on HRCT, presence or absence of preoperative diagnosis, operation procedures, observation period, pathological parameters, months of postoperative administration of oral anti-cancer agent such as uracil-tegafur if used, presence or absence of cancer recurrence, and some other additional information. The initial recurrence sites were also investigated in cancer relapsed cases. Comparisons were performed between Group 1 and Group 2 in both all-NSCLC (n = 179) and adenocarcinoma specified subset (n = 151).
For the statistical analysis, Fisher’s exact test was used to compare proportional values, and nonparametric Mann–Whitney’s U test was used to compare continuous values between Group 1 and Group 2. For propensity matching, each propensity score was derived as ‘expected probability’ for the ‘presence of preoperative bronchoscopic cancer confirmation’ calculated by binary logistic regression model. Covariates used in that model were age, gender, radiological tumor larger diameters and solid portion diameter, and pathological diameter.
Matched pairs were made by propensity caliper matching method, in which every single difference of propensity scores was no more than 0.011. For all-NSCLC cohort, 96 cases (48 pairs) were matched, and for adenocarcinoma subset, 82 cases (41 pairs) were matched. Subsequently, Kaplan–Meier method with log-rank test was performed on groups of matched pairs, and Cox proportional hazard model analysis was performed on whole matched cases.
In the Cox model, covariates used were age, gender, tumor longer diameter on HRCT, solid portion diameter on HRCT, presence of preoperative bronchoscopic cancer confirmation (equal to belonging to Group 1), and months of oral uracil-tegafur administration. Validation of Cox proportional hazard model was obtained by log-minus-log graphs in which both groups made parallel curves when validated. Bilateral standard of p < 0.05 was regarded significant in each statistical test. All statistical analysis was performed on the statistical software Dr. SPSS II (IBM analytics, USA).
Results
Of all 179 selected NSCLC patients, 151 (84%) were adenocarcinoma. Rest 28 cases were: 19 (11%) squamous cell carcinoma; 6 (4%) large cell carcinoma; and 3 (2%) adenosquamous carcinoma. All tumors were located outer half of the lung periphery in accordance with inclusion criteria.
Preoperative bronchoscope was performed in all 179 NSCLC; 110 cases underwent both brushing cytology and TBB; 66 cases underwent brushing cytology only; and 3 with TBB only. Transbronchial needle aspiration was cooperatively performed with brushing or TBB in 6 patients. Of 179 those bronchoscope performed cases, 95 had successful cancer confirmation (overall diagnostic yield of bronchoscope was 53%). Cytological cancer confirmation was made in accordance with typical 5-grade classification, and both class 4 and class 5 were regarded cytological positive, while class 1, class 2, and class 3 were judged as negative. Diagnostic yields did not differ between adenocarcinoma subset (53%) and non-adenocarcinoma NSCLC (54%). Endobronchial ultrasonography and guide sheath (EBUS-GS) was used in 57 (32%) of 179 bronchoscope performed cases, and its diagnostic yield was 72% which was much higher than that of non-EBUS-GS of 44% (p = 0.0005).
After all, 95 cases with successful bronchoscopic cancer confirmation were assigned to Group 1. Rest 84 cases with failed result of bronchoscopic cancer confirmation were assigned to Group 2.
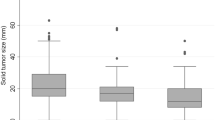
Population, size, and solid portion proportion by tumor location are shown in Table 1. There seems to be obvious tendency that Group 1 had larger tumors than Group 2.
There were significant differences regarding several variates between Group 1 and Group 2 of all-NSCLC before propensity matching (Table 2, left): male, tumor longer diameter, solid portion diameter, and vascular involvement were all dominant in Group 1 of all-NSCLC. When cases were matched (48 cases versus 48 cases), between-group differences were well balanced in all variates which were adopted in generating propensity score (Table 2, right), and Kaplan–Meier curves revealed no difference between Group 1 and Group 2 regarding RFS of all-NSCLC (Fig. 1, left). Cox proportional hazard model showed that no covariates other than ‘solid portion diameter’ and ‘postoperative oral uracil-tegafur’ had significant hazard ratio (HR) for cancer recurrence in all-NSCLC (Fig. 2, upper).

Recurrence-free survivals of propensity score matched Group 1 and Group 2 in all-NSCLC and in adenocarcinoma subset

Results of Cox proportional hazard model analysis for the risk of cancer recurrence after propensity score matching
When the cohort was specified to adenocarcinoma, similar to all-NSCLC, there were significant differences in several variates between non-matched groups (Table 3, left): male, tumor longer diameter, solid portion diameter, and vascular involvement were dominant in Group 1. When cases were matched (41 cases versus 41 cases), between-group differences were fairly adjusted in all variates, as well (Table 3, right). Log-rank test also revealed no significant difference regarding RFS between Group 1 and Group 2 (Fig. 1, right). Cox proportional hazard model with matched cases revealed no covariate including ‘presence of bronchoscopic cancer confirmation’ which was a risk factor for adenocarcinoma recurrence (Fig. 2, lower).
Table 4 shows a comparison of primary affected organs in adenocarcinoma recurred cases. There was no specific distribution of initial recurrence site in between matched Group 1 and Group 2 of adenocarcinoma. We found that lung metastasis and pleural dissemination might be slightly dominant in Group 1; however, numbers of cases were too small to be valid.
Discussion
This study was particularly designed to examine a statistical significance of possible predictor which has been rarely considered to be a risk of lung cancer recurrence. Initially, our aim was to investigate whether ‘attempting diagnostic bronchoscope’ would affect patients’ prognosis. However, when we made a preparatory exploring analysis using non-adjusted primary data set of 227 stage1A resected NSCLC patients, it was revealed that attempting bronchoscope itself might not be a predictor for cancer recurrence; however, ‘cancer confirmation by bronchoscope’ had only significant hazard ratio of 3.29 (Table 5). Therefore, we had changed the study purpose to find ‘bronchoscopic cancer confirmation’ which would work unfavorably on cancer recurrence.
Because studies based on lower population could not generate enough statistical power [7], we have to adjust biases as far as possible to maximize study sensitivity. In our study, like other studies concerning to lung cancer predictors, tumor size had become the most non-negligible bias. That is, because smaller tumors would be easy to be failed to cancer diagnosis, cases with such small nodules tended to be assigned to Group 2. This aspect would be totally correct, because tumor sizes of Group 1 seemed to be 0.2–0.3 cm larger than those of Group 2 (Table 1). Under this situation, propensity score matching method worked well in balancing such size-based bias, and ultimately, preferable matched pairs could be obtained (Fig. 2).
In addition, in the preparatory analysis, we found that there would be little statistical difference in cancer recurrence rate when biological high grade malignancy such as pleural involvement and nodal involvement were included. This might be due to that iatrogenic factor affected lesser on their prognosis than natural biological factors did, and almost of such small effect would have been fully offset and submerged. Both pleural involvement and nodal involvement are such strong predictors that they can define pathological stage independently [7, 8]; we limited those two factors to ‘no involvement’ in our study.
As a result, each matched group in NSCLC and adenocarcinoma subset had highly similar basis, so the results subsequently derived from Kaplan–Meier method or Cox proportional hazard model would be fairly reliable [9]. For the validation, we performed an alternative propensity method (i.e., propensity calibration method [10]) on the non-matched dataset, in which we found almost the same result as the main analysis.
Tumor size is one of the most strong predictors in general [11,12,13]; however, we found that tumor longer diameter had minimal impact on risk for cancer recurrence at least in the examined range in our study. Recent studies suggested that solid portion diameter (especially in invasive lepidic adenocarcionoma) on HRCT would be more important than tumor longer diameter for the prognosis of adenocarcinoma [14], and such a concept was similarly adopted in new (version 8) Tumor, Node, and Metastasis staging system of Union for International Cancer Control [8]. Similarly, in our model, we found that solid portion diameter affects increase of recurrence risk even in our limited cohorts. In addition, in a preparatory multivariate analysis, using non-size-adjusted 227 stage1A NSCLC cases, when we excluded iatrogenic factors listed on Table 5 (i.e., ‘cancer confirmation by bronchoscope’, ‘preoperative bronchoscope’ and ‘postoperative uracil-tegafur administration’), we found that ‘solid portion diameter’ was emerged as a significant predictor (HR 1.18, 95% CI 1.07–1.32) instead of ‘longer diameter’ (HR 0.91, 95% CI 0.79–1.06).
For the predictors such as lymphatic and vessel involvement, present evaluation method by hematoxylin–eosin stain specimen is regarded inaccurate according to a recent study [15]. In fact, we found so scattered and deviated pathological reports were made regarding above two factors in our institution. In addition, even if their status could affect outcomes, we cannot distinguish whether their status was caused by natural biological behavior, or by preoperative bronchoscopic laceration of tumor vessels or lympatics. Therefore, it was considered inappropriate to adopt them as covariates both in calculating propensity score and in further multivariate analysis.
Use of postoperative oral anti-cancer agents was a major possible prognostic factor to be considered. Of these, postoperative oral uracil-tegafur administration for surgically resected stage 1A and 1B NSCLC is locally practiced intervention only prevailed in Japan based on two major studies [16, 17]. In our model, postoperative uracil-tegafur administration revealed rather poorer effect on prognosis of stage 1A NSCLC.
As for iatrogenic factors which were not adopted as covariates in our study, ‘extent of resection’, and ‘degrees of nodal dissection’, ‘use of video-assisted thoracoscopic surgery’ should have been also considered, and all of them were unified in the case selection. In addition, because no patients had been given other adjuvant chemotherapy than uracil-tegafur administration, nothing would be remained as potent predictor which would affect cancer recurrence in this study.
If it is the case that bronchoscopic cancer confirmation is an unfavorable prognostic factor, distant metastasis or lymph node metastasis might be dominant in group 1, because laceration of tumor vessels or lymphatics would be caused by bronchoscopic manipulations. However, we found little difference between Group 1 and Group 2 regarding the initial recurrent site. Instead, lung metastasis and pleural dissemination had slightly dominant tendencies in Group 1, to which we could not give a good explanation.
As the report from the Japanese lung cancer registry showed a significant prognostic inferiority of non-adenocarcinoma NSCLC comparted to adenocarcinoma [18], non-adenocarcinoma subset might contain biologically malignant characters enough to offset small iatrogenic effects. However, the same results between all-NSCLC and adenocarcinoma subset were obtained in this study.
With all these aspects, we found preoperative bronchoscopic cancer confirmation does not increase recurrence risk in stage1A NSCLC in this study. Though much larger prospective study would be warranted to varify, we can conclude that we should not have a threat for increasing risk of recurrence by preoperative bronchoscopic cancer comfirmation. To our knowledge, this is the first-ever report which denies risk of preoperative bronchoscope for lung cancer recurrence.
Abbreviations
- CI:
-
Confidence interval
- EBUS-GS:
-
Endobronchial ultrasonography-guide sheath
- HR:
-
Hazard ratio
- HRCT:
-
High-resolution computed tomography
- LLL:
-
Left lower lobe
- LUL:
-
Left upper lobe
- NSCLC:
-
Non-small cell lung cancer
- RFS:
-
Recurrence-free survival
- RLL:
-
Right lower lobe
- RML:
-
Right middle lobe
- RUL:
-
Right upper lobe
- TBB:
-
Transbronchial biopsy
References
Kurimoto N, Miyazawa T, Okimasa S, et al. Endobronchial ultrasonography using a guide sheath increases the ability to diagnose peripheral pulmonary lesions endoscopically. Chest. 2004;126(3):959–65.
Asano F, Matsuno Y, Matsushita T, et al. Transbronchial diagnosis of a small peripheral pulmonary lesion using an ultrathin bronchoscope with virtual bronchoscopic navigation. J Bronchol. 2002;9:108–11.
Shinagawa N, Yamazaki K, Onodera Y, et al. CT-guided transbronchial biopsy using an ultrathin bronchoscope with virtual bronchoscopic navigation. Chest. 2004;125(3):1138–43.
Sawabata N, Ohta M, Maeda H. Fine-needle aspiration cytologic technique for lung cancer has a high potential of malignant cell spread through the tract. Chest. 2000;118(4):936–9.
Nakajima J, Sato H, Takamoto S. Dose preoperative transbronchial biopsy worsen the postsurgical prognosis of lung cancer? A propensity score-adjusted analysis. Chest. 2005;128(5):3512–8.
Sawabata N, Maeda H, Ohta M, Hayakawa M. Operable non-small cell lung cancer diagnosed by transpleural techniques: do they affect relapse and prognosis? Chest. 2001;120(5):1595–8.
Brundage MD, Davies D, Mackillop WJ. Prognostic factors in non-small cell lung cancer. Chest. 2002;122(3):1037–57.
Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11(1):39–51.
Austin PC. Propensity-score matching in the cardiovascular surgery literature from 2004 to 2006: a systematic review and suggestions for improvement. J Thorac Cardiovasc Surg. 2007;134(5):1128–35.
Stürmer T, Schneeweiss S, Rothman KJ, Avorn J, Glynn RJ. Performance of propensity score calibration—a simulation study. Am J Epidemiol. 2007;165(10):1110–8.
Koike T, Terashima M, Takizawa T, Watanabe T, Kurita Y, Yokoyama A. Clinical analysis of small-sized peripheral lung cancer. J Thorac Cardiovasc Surg. 1998;115(5):1015–20.
Zhu WY, Tan LI, Wang ZY, et al. Clinical characteristics and advantages of primary peripheral microsized lung adenocarcinoma over small-sized lung adenocarcinoma. Eur J Cardiothorac Surg. 2016;49:1095–102.
Maeda R, Yoshida J, Ishii G, et al. Long-term survival and risk factors for recurrence in stage I non-small cell lung cancer patients with tumors up to 3 cm in maximum dimension. Chest. 2010;138(2):357–62.
Borczuk AC, Qian F, Kazeros A, et al. Invasive size is an independent predictor of survival in pulmonary adenocarcinoma. Am J Surg Pathol. 2009;33(3):462–9.
Okada S, Mizuguchi S, Izumi N, et al. Prognostic value of the frequency of vascular invasion in stage 1 non-small cell lung cancer. Gen Thorac Cardiovasc Surg. 2017;65(1):32–9.
Kato H, Ichinose Y, Ohta M, et al. A randomized trial of adjuvant chemotherapy with uracil-tegafur for adenocarcinoma of the lung. N Engl J Med. 2004;350(17):1713–21.
Hamada C, Tsuboi M, Ohta M, et al. Effect of postoperative adjuvant chemotherapy with tegafur-uracil on survival in patients with stage 1A non-small cell lung cancer. J Thorac Oncol. 2009;4(12):1511–6.
Asamura H, Goya T, Koshiishi Y, et al. A Japanese lung cancer registry study. J Thorac Oncol. 2008;3(1):46–52.
Acknowledgements
For this publication, each author had engaged in the work as follows; Jiro Abe designed the study structure, collected patients’ data, analyzed data, and wrote the article; Toshimasa Okazaki collected patients’ data; Naohiko Kikuchi collected patients’ data; Satomi Takahashi collected patients’ data; Akira Sakurada advised regarding statistical issue; Yoshinori Okada supervised the whole work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Rights and permissions
About this article

Cite this article
Abe, J., Okazaki, T., Kikuchi, N. et al. Preoperative bronchoscopic cancer confirmation does not increase risk of recurrence in stage1A non-small cell lung cancer. Gen Thorac Cardiovasc Surg 66, 284–290 (2018). https://doi.org/10.1007/s11748-018-0909-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-018-0909-y