
Abstract
Objective
Despite excellent long-term results reported for a trans-aortic septal myectomy for hypertrophic obstructive cardiomyopathy (HOCM), surgery for patients with diffuse hypertrophy is very challenging. In addition, a left ventricular outflow obstruction is often aggravated by an abnormal mitral valve and subvalvular apparatus.
Methods
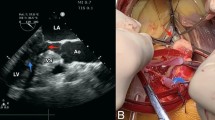
We performed video-assisted minimally invasive trans-mitral septal myectomy procedures in 3 patients with diffuse-type HOCM, who were highly symptomatic despite maximal medical therapy. Each had at least moderate mitral regurgitation (MR) due to systolic anterior motion (SAM). Using a right mini-thoracotomy, the anterior mitral leaflet was detached, through which an extended septal myectomy could easily be performed. Abnormal bridging chordae between the septum and papillary muscle (PM) were divided, then anterior mitral leaflet continuity was restored with direct closure or augmentation using a glutaraldehyde-treated autologous pericardium. A PM reorientation procedure was performed in 1 case in which both PMs were approximated and sutured onto the posterior ventricular wall.
Results
The postoperative course was uneventful in all patients, with marked improvement of symptoms in each. The peak ventricular outflow gradient decreased from 134 ± 40 to 23 ± 5 mmHg with significantly diminished SAM, especially in the patient who underwent the PM reorientation procedure. During a mean follow-up period of 42 ± 14 months, no MR has been detected in any case.
Conclusions
We believe that a minimally invasive trans-mitral septal myectomy is preferable for HOCM-patients with diffuse hypertrophy and mitral valve abnormality. Aggressive PM reorientation may also be useful for those with an abnormal PM orientation.





Similar content being viewed by others


References
Dearani JA, Ommen SR, Gersh BJ, Schaff HV, Danielson GK. Surgery insight: septal myectomy for obstructive hypertrophic cardiomyopathy—the Mayo Clinic experience. Nat Clin Plact Cardiovasc Med. 2007;4:503 – 12.
Sherrid MV, Balaram S, Kim B, Axel L, Swistel DG. The mitral valve in obstructive hypertrophic cardiomyopathy. A test in context. J Am Coll Cardiol. 2016;67:1846–58.
Matsuda H, Nomura F, Kadoba K, Taniguchi K, Imagawa H, Kagisaki K, et al. Transatrial and transmitral approach for left ventricular myectomy and mitral valve plication for diffuse-type hypertrophic obstructive cardiomyopathy: a novel approach. J Thorac Cardiovasc Surg. 1996;112:195–6.
Gutermann H, Pettinari M, Van Kerrebroeck C, Laenen MV, Engelen K, Fret T, et al. Myectomy and mitral repair through the left atrium in hypertrophic obstructive cardiomyopathy: the preferred approach for contemporary surgical candidates? J Thorac Cardiovasc Surg. 2014;147:1833–6.
Kudo M, Yozu R, Kokaji K, Kimura N. A simple method of prevention for systolic anterior motion in mitral valve repair by loop technique method. Ann Thorac Surg. 2009;87:324–5.
Casselman F, Vanermen H. Idiopathic hypertrophic subaortic stenosis can be treated endoscopically. J Thorac Cardiovasc Surg. 2002;124:1248–9.
Klues HG, Maron BJ, Dollar AL, Roberts WC. Diversity of structural mitral valve alterations in hypertrophic cardiomyopathy. Circulation. 1992;85:1651–60.
Balaram SK, Ross RE, Sherrid MV, Schwartz GS, Hillel Z, Winson G, et al. Role of mitral valve plication in the surgical management of hypertrophic cardiomyopathy. Ann Thorac Surg. 2012;94:1990–8.
Mascagni R, Attar NA, Lamarra M, Calvi S, Tripodi A, Mebazaa A, et al. Edge-to-edge technique to treat post-mitral valve repair systolic anterior motion and left ventricular outflow tract obstruction. Ann Thorac Surg. 2005;79:471–4.
Vriesendorp PA, Schinkel AFL, Soliman OII, Kofflard MJM, de Jong PL, can Herwerden LA, et al. Long-term benefit of myectomy and anterior mitral leaflet extension in obstructive hypertrophic cardiomyopathy. Am J Cardiol. 2015;115:670 – 75.
Klues HG, Roberts WC, Maron BJ. Anomalous insertion of papillary muscle directly into anterior mitral leaflet in hypertrophic cardiomyopathy. significance in producing left ventricular outflow obstruction. Circulation. 1991;84:1188–97.
Seeburger J, Passage J, Borger MA, Mohr FW. A new concept for correction of systolic anterior motion and mitral valve regurgitation in patients with hypertrophic obstructive cardiomyopathy. J Thorac Cardiovasc Surg. 2010;140:481–3.
Ferrazzi P, Spirito P, Iacovoni A, Calabrese A, Migliorati K, Simon C, et al. Transaortic chordal cutting. Mitral valve repair for obstructive hypertrophic cardiomyopathy with mild septal hypertrophy. J Am Coll Cardiol. 2015;66:1687–96.
Bryant R 3rd, Smedira NG. Papillary muscle realignment for symptomatic left ventricular outflow tract obstruction. J Thorac Cardiovasc Surg. 2008;135:223–4.
Kwon DH, Smedira NG, Thamilarasan M, Lytle BW, Lever H, Desai MY. Characteristics and surgical outcomes of symptomatic patients with hypertrophic cardiomyopathy with abnormal papillary muscle morphology undergoing papillary muscle reorientation. J Thorac Cardiovasc Surg. 2010;140:317 – 24.
Hong JH, Schaff HV, Nishimura RA, Abel MD, Derarani JA, Li Z, et al. Mitral regurgitation in patients with hypertrophic obstructive cardiomyopathy. Implications for concomitant valve procedures. J Am Coll Cardiol. 2016;68:1497 – 504.
Shomura Y, Okada Y, Nasu M, Koyama T, Yuzaki M, Murashita T, et al. Late results of mitral valve repair with glutaraldehyde-treated autologous pericardium. Ann Thorac Surg. 2013;95:2000–6.
Fukunaga N, Matsuo T, Saji Y, Imai Y, Koyama T. Mitral valve stenosis progression due to severe calcification on glutaraldehyde-treated autologous pericardium: word of caution for an attractive repair technique. Ann Thorac Surg. 2015;99:2203–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author has declared that no conflict of interest exists.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 7 (MPG 1464 KB)
Supplementary material 8 (MPG 1061 KB)
Rights and permissions
About this article

Cite this article
Sakaguchi, T., Totsugawa, T., Tamura, K. et al. Minimally invasive trans-mitral septal myectomy for diffuse-type hypertrophic obstructive cardiomyopathy. Gen Thorac Cardiovasc Surg 66, 321–326 (2018). https://doi.org/10.1007/s11748-018-0908-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-018-0908-z