
Abstract
Background
Extended arch repair for acute type A aortic dissection remains controversial. Our strategy for acute type A aortic dissection was primary entry resection and tear-oriented ascending/hemiarch replacement for patients with the intimal tear in the ascending aorta or is not found in the ascending/aortic arch. Extended total/partial arch replacement was performed for patients with the tear located in the aortic arch. Here, we investigated the validity of our strategy from the viewpoints of long-term survival and reoperation.
Patients and methods
Between 2003 and 2014, 267 acute type A aortic dissection patients (mean age; 65.2 ± 12.9 years, 134 men and 133 women) underwent emergent surgical repair. Ascending/hemiarch replacements were performed in 225 patients (ascending/hemiarch group) and total/partial arch replacements in 42 patients (arch group). Early and late outcomes of both groups were compared.
Results
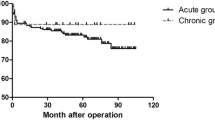
The hospital mortality rates in the ascending/hemiarch and the arch groups were 4.4 and 9.5 %, respectively (p = 0.25). For ascending/hemiarch and arch groups, the actuarial survival rates were 80.7 vs. 84.3 % after 5 years, and 66.4 vs. 74.6 %, respectively, after 10 years (p = 0.94). For ascending/hemiarch and arch groups, reoperation-free survival rates were 72.1 vs. 77.1 % after 5 years, and 62.0 vs. 67.1 %, respectively, after 10 years (p = 0.85).
Conclusions
We observed no significant differences in the actuarial survival or reoperation-free survival rates between the groups. These findings suggest that tear-oriented ascending/hemiarch replacement for acute type A aortic dissection does not increase the risk of long-term mortality or reoperation.


Similar content being viewed by others


References
Kimura N, Itoh S, Yuri K, Adachi K, Matsumoto H, Yamaguchi A, et al. Reoperation for enlargement of the distal aorta after initial surgery for acute type A aortic dissection. J Thorac Cardiovasc Surg. 2015;149:S91–8.
Kimura N, Tanaka M, Kawahito K, Yamaguchi A, Ino T, Adachi H. Influence of patent false lumen on long-term outcome after surgery for acute type A aortic dissection. J Thorac Cardiovasc Surg. 2008;136:1160–6.
Zierer A, Voeller RK, Hill KE, Kouchoukos NT, Damiano Jr RJ, Moon MR. Aortic enlargement and late reoperation after repair of acute type A aortic dissection. Ann Thorac Surg. 2007;84:479–86 (discussion 486–7).
Uchida N, Shibamura H, Katayama A, Shimada N, Sutoh M, Ishihara H. Operative strategy for acute type a aortic dissection: ascending aortic or hemiarch versus total arch replacement with frozen elephant trunk. Ann Thorac Surg. 2009;87:773–7.
Takahara Y, Sudo Y, Mogi K, Nakayama M, Sakurai M. Total aortic arch grafting for acute type A dissection: analysis of residual false lumen. Ann Thorac Surg. 2002;73:450–4.
Kazui T, Washiyama N, Muhammad BA, Terada H, Yamashita K, Takinami M, et al. Extended total arch replacement for acute type a aortic dissection: experience with seventy patients. J Thorac Cardiovasc Surg. 2000;119:558–65.
Urbanski PP, Siebel A, Zacher M, Hacker RW. Is extended aortic replacement in acute type A dissection justifiable? Ann Thorac Surg. 2003;75:525–9.
Westaby S, Saito S, Katsumata T. Acute type A dissection: conservative methods provide consistently low mortality. Ann Thorac Surg. 2002;73:707–13.
Shiono M, Hata M, Sezai A, Niino T, Yagi S, Negishi N. Validity of a limited ascending and hemiarch replacement for acute type A aortic dissection. Ann Thorac Surg. 2006;82:1665–9.
Tanaka M, Kimura N, Yamaguchi A, Adachi H. In-hospital and long-term results of surgery for acute type A aortic dissection: 243 consecutive patients. Ann Thorac Cardiovasc Surg. 2012;18:18–23.
Omura A, Miyahara S, Yamanaka K, Sakamoto T, Matsumori M, Okada K, et al. Early and late outcomes of repaired acute DeBakey type I aortic dissection after graft replacement. J Thorac Cardiovasc Surg. 2015;151:341–8.
Conzelmann LO, Weigang E, Mehlhorn U, Abugameh A, Hoffman I, Blettner M, et al. Mortality in patients with acute aortic dissection type A: analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur J Cardiothorac Surg. 2016;49:e44–52.
Yan Y, Xu L, Zhang H, Xu ZY, Ding XY, Wang SW, et al. Proximal aortic repair versus extensive aortic repair in the treatment of acute type A aortic dissection: a meta-analysis. Eur J Cardiothorac Surg. 2015;. doi:10.1093/ejcts/ezv351.
Rylski B, Beyersdorf F, Kari FA, Schlosser J, Blanke P, Siepe M. Acute type A aortic dissection extending beyond ascending aorta: Limited or extensive distal repair. J Thorac Cardiovasc Surg. 2014;148:949–54 (discussion 954).
Luciani N, De Geest R, Lauria G, Farina P, Luciani M, Glieca F, et al. Late reoperations after acute aortic dissection repair: single-center experience. Asian Cardiovasc Thorac Ann. 2015;23:787–94.
Uchida N. Open stent grafting for complex diseases of the thoracic aorta: clinical utility. Gen Thorac Cardiovasc Surg. 2013;61:118–26.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Kei Aizawa and other coauthors have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Rights and permissions
About this article

Cite this article
Aizawa, K., Kawahito, K. & Misawa, Y. Long-term outcomes of tear-oriented ascending/hemiarch replacements for acute type A aortic dissection. Gen Thorac Cardiovasc Surg 64, 403–408 (2016). https://doi.org/10.1007/s11748-016-0648-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-016-0648-x