
Abstract
Background
Thoracoscopic esophagectomy for esophageal cancer performed using two-lung ventilation in the prone position has many advantages, such as convenient anesthesia induction and maintenance, and good oxygenation. We examined the safety of surgery and anesthetic management by following chronological changes in intraoperative respiration and hemodynamics.
Methods
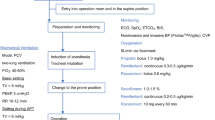
We focused on the most recent and consecutive 14 cases of thoracoscopic esophagectomy for esophageal cancer in the prone position performed from November 2010 until recently. We measured the following items by use of FloTrac system : cardiac index (CI), central venous pressure (CVP), mean arterial pressure, partial pressure of oxygen in arterial blood (PaO2), partial pressure of carbon dioxide in arterial blood (PaCO2), peak airway pressure (APmax), and tidal volume.
Results
No major changes were observed in CI, systolic blood pressure, and TV after the start of pneumothorax (statically not significant). Conversely, CVP increased immediately after pneumothorax (p < 0.05) and decreased almost to its original level thereafter. The mean APmax value was 18–20 cm H2O [mean increase, 4.2 cm H2O; (p < 0.05)]. The mean P/F ratio and mean PaCO2 were 244.4 and 48.3 mmHg, respectively, during artificial pneumothorax.
Conclusion
No excessive increases in airway pressure or clear circulatory depressions were observed because of artificial pneumothorax under two-lung ventilation in thoracoscopic esophagectomy for esophageal cancer in the prone position. These results suggest that artificial pneumothorax under two-lung ventilation is beneficial for maintaining stable hemodynamics and oxygenation in thoracoscopic esophagectomy in prone position.










Similar content being viewed by others


References
Palanivelu C, Prakash A, Senthikumar R, Senthilnathan P, Parthasarathi R, Rajan PS, et al. Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position–experience of 130 patients. J Am coll Surg. 2006;203:7–16.
Jones DR, Graeber GM, Tanguiling GG, Hobbs G. Murray: effects of insufflation on hemodynamics during thoracoscopy. Ann Thorac Surg. 1993;55:1379–82.
Sato M, Muraji T, Asai T, Hamada Y, Hioki K. Hemodynamic effects of carbon dioxide insufflation of the thoracic cavity during thoracoscopic surgery. Padiatr Endosurg Innov Tech. 2002;6:185–9.
Hill RC, Jones DR, Vance RA, Behrooz K. Selective lung ventilation during thoracoscopy: effects of insufflation on hemodynamics. Ann Thorac Surg. 1996;61:945–8.
Wolfer RS, Krasna MJ, Hasnain JU, McLaughlin JS. Hemodynamic effects of carbon dioxide insufflation during thoracoscopy. Ann Thorac Surg. 1994;58:404–8.
Schwarzkopf K, Klein U, Schreiber NP, Bloos F, Helfritsch H, Sauer F, et al. Oxygenation during one-lung ventilation: the effect of inhaled nitric oxide and increasing levels of inspired fraction of oxygen. Anesth Analg. 2001;92:842–7.
Cohen E, Eisenkraft JB, Thys DM, Kirschner PA, Kaplan JA. Oxygenation and hemodynamic changes during one-lung ventilation: effects of CPAP10, PEEP10, andCPAP/PEEP10. J Cardiothoracic Anesth. 1988;2:34–40.
Fujiwara M, Abe Kazuo, Mashimo T. The effect of positive end-expiratory pressure and continuous positive airway pressure on the oxygenation and shunt fraction during one-lung ventilation with propofol anesthesia. J Clin Anesth. 2001;13:473–7.
Kim YD, Ko S, Kim D, Lim H, Lee JH, Kim MH. The effects of incremental continuous positive airway pressure on arterial oxygenation and pulmonary shunt during one-lung ventilation. Korean J Anesthesiol. 2012;62:256–9.
Ishikawa S, Nakazawa K, Makita K. Progressive changes in arterial oxygenation during one-lung anaesthesia are related to the response to compression of the non-dependent lung. Br J Anaesth. 2003;90:21–6.
Conflict of interest
We have not received any funds for the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Saikawa, D., Okushiba, S., Kawata, M. et al. Efficacy and safety of artificial pneumothorax under two-lung ventilation in thoracoscopic esophagectomy for esophageal cancer in the prone position. Gen Thorac Cardiovasc Surg 62, 163–170 (2014). https://doi.org/10.1007/s11748-013-0335-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-013-0335-0