
Abstract
Purpose
There is no recommended standard follow-up program after resection for lung cancer. Under these circumstances, each doctor establishes his or her own follow-up protocol. This questionnaire survey was conducted to grasp the current status of postoperative follow-up in Japan.
Methods
The questionnaire survey was aimed at determining what examinations were performed and at what frequencies in the setting of postoperative follow-up. Based on these results, examinations performed at a frequency of >50% and the time points after resection at which they were performed were selected and presented as components of an average follow-up program.
Results
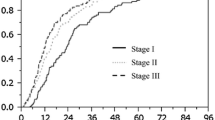
Questionnaires were sent to 44 institutions, and 26 doctors responded to the questionnaire. All 26 of the doctors performed physical examinations, blood examinations, chest radiography, and computed tomography (CT) routinely, but their frequencies varied widely among the doctors. The average frequencies of the follow-up examinations as judged from this survey are as follows: Physical and blood examinations are performed three to four times a year for the first 3 years and twice a year during the next 2 years. CT is scheduled at 6 and 12 months after resection and is repeated annually thereafter. Chest radiography is performed three to four times a year for the first 3 years and once a year thereafter, between the CT examinations.
Conclusion
The follow-up programs used in clinical practice vary widely among institutions and doctors in terms of the types of examination performed and the frequencies at which they are performed.
Similar content being viewed by others

References
Asamura H, Goya T, Koshiishi Y, Sohara Y, Eguchi K, Mori M, et al. A Japanese Lung Cancer Registry study: prognosis of 13,010 resected lung cancers. J Thorac Oncol 2008;3:46–52.
Chiu CH, Chern MS, Wu MH, Hsu WH, Wu YC, Huang MH, et al. Usefulness of low-dose spiral CT of the chest in regular follow-up of postoperative non-small cell lung cancer patients: preliminary report. J Thorac Cardiovasc Surg 2003;125:1300–1305.
Westeel V, Choma D, Clement F, Woronoff-Lemsi MC, Pugin JF, Dubiez A, et al. Relevance of an intensive postoperative follow-up after surgery for non-small cell lung cancer. Ann Thorac Surg 2000;70:1185–1190.
Egermann U, Jaeggi K, Habicht JM, Perruchoud AP, Dalquen P, Soler M. Regular follow-up after curative resection of nonsmall cell lung cancer: a real benefit for patients? Eur Respir J 2002;19:464–468.
Walsh GL, O’Connor M, Willis KM, Milas M, Wong RS, Nesbitt JC, et al. Is follow-up of lung cancer patients after resection medically indicated and cost-effective? Ann Thorac Surg 1995;60:1563–1570; discussion 1570–2.
Younes RN, Gross JL, Deheinzelin D. Follow-up in lung cancer: how often and for what purpose? Chest 1999;115:1494–1499.
Virgo KS, Naunheim KS, McKirgan LW, Kissling ME, Lin JC, Johnson FE. Cost of patient follow-up after potentially curative lung cancer treatment. J Thorac Cardiovasc Surg 1996;112:356–363.
Virgo KS, McKirgan LW, Caputo MC, Mahurin DM, Chao LC, Caputo NA, et al. Post-treatment management options for patients with lung cancer. Ann Surg 1995;222:700–710.
Japanese Lung Cancer Society. Japanese clinical practice guideline for lung cancer. Kanehara Shuppan, 2005.
Sobin L, Wittekind, C. UICC TNM classification of malignant tumors. 6th edn, New York: Wiley-Liss, 2002. p. 272.
Anonymous. Follow-up of non-small lung cancer. American College of Radiology appropriateness criteria, 2005–2007. Available at: www.acr.org.
Rubins J, Unger M, Colice GL. Follow-up and surveillance of the lung cancer patient following curative intent therapy: ACCP evidence-based clinical practice guideline (2nd edition). Chest 2007;132(suppl):355S–367S.
Felip E, Stahel RA, Pavlidis N. ESMO Minimum clinical recommendations for diagnosis, treatment and follow-up of non-small-cell lung cancer (NSCLC). Ann Oncol 2005;16(suppl 1):i28–i29.
Pfister DG, Johnson DH, Azzoli CG, Sause W, Smith TJ, Baker S Jr, et al. American Society of Clinical Oncology treatment of unresectable non-small-cell lung cancer guideline: update 2003. J Clin Oncol 2004;22:330–353.
Takenaka D, Ohno Y, Koyama H, Nogami M, Onishi Y, Matsumoto K, et al. Integrated FDG-PET/CT vs. standard radiological examinations: comparison of capability for assessment of postoperative recurrence in non-small cell lung cancer patients. Eur J Radiol 2010;74:458–464.
Hicks RJ, Kalff V, MacManus MP, Ware RE, McKenzie AF, Matthews JP, et al. The utility of (18)F-FDG PET for suspected recurrent non-small cell lung cancer after potentially curative therapy: impact on management and prognostic stratification. J Nucl Med 2001;42:1605–1613.
Hellwig D, Groschel A, Graeter TP, Hellwig AP, Nestle U, Schafers HJ, et al. Diagnostic performance and prognostic impact of FDG-PET in suspected recurrence of surgically treated non-small cell lung cancer. Eur J Nucl Med Mol Imaging 2006;33:13–21.
Keidar Z, Haim N, Guralnik L, Wollner M, Bar-Shalom R, Ben-Nun A, et al. PET/CT using 18F-FDG in suspected lung cancer recurrence: diagnostic value and impact on patient management. J Nucl Med 2004;45:1640–1646.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sawada, S., Suehisa, H., Yamashita, M. et al. Current status of postoperative follow-up for lung cancer in Japan: questionnaire survey by the Setouchi Lung Cancer Study Group—A0901. Gen Thorac Cardiovasc Surg 60, 104–111 (2012). https://doi.org/10.1007/s11748-011-0850-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-011-0850-9