
Abstract
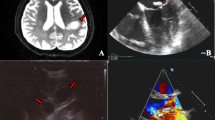
The proper management of a patient with active infective endocarditis (IE) remains to be determined, especially when his or her condition is complicated with intracranial mycotic aneurysm. Here we present a 46-year-old company employee hospitalized with a subarachnoid hemorrhage caused by a ruptured mycotic aneurysm. Cardiac echography showed a verruca on the posterior mitral cusp and leaflet destruction, resulting in severe valvular regurgitation (determined pathogen was α-streptococcus). High-dose antibiotic infusion and restriction of physical activity to prevent heart failure were combined with emergency craniotomy drainage and coiling of the necks of two cerebral mycotic aneurysms. After 2 months of conservative therapy for IE, he suddenly collapsed with hypotension and bradycardia because of embolic occlusion of the proximal right coronary artery (RCA). An emergent operation was carried out to remove the emboli in the RCA and to replace the mitral valve with a mechanical prosthesis. The postoperative course was uneventful. Although disturbances of spatial recognition and manual dexterity remained, he was able to walk and talk. After postoperative sufficient-duration antibiotic therapy, which lasted 20 days, he was transferred to a rehabilitation center.
Similar content being viewed by others


References
Snygg-Martin U, Gustafsson L, Rosengren L, Alsiö A, Ackerholm P, Andersson R, et al. Cerebrovascular complications in patients with left-sided infective endocarditis are common; a progressive study using magnetic resonance imaging and neurochemical brain damage markers. Clin Infect Dis 2008;47:23–30.
Hart RG, Kagan-Hallet K, Joerns SE. Mechanisms of intracranial hemorrhage in infective endocarditis. Stroke 1987;18:1048–1056.
Yamasaki M, Watanabe S, Abe K, Uenishi M, Kawazoe K. Successful surgical treatment with mitral valve replacement and coronary embolectomy in a patient with active endocarditis complicated with multi septic embolism involving cerebral arteries and right coronary artery. Gen Thorac Cardiovasc Surg 2010; in press.
Miyatake K, Akaishi M, Ishizuka N, Eishi K, Kawazoe K, Nakazawa M, et al. The Japanese Circulation Society: guidelines for the prevention and treatment of infective endocarditis (http://www.j-circ.or.jp/guideline/index.htm). accessed 23 October 2009.
Eishi K, Kawazoe K, Kuriyama Y, Kitoh Y, Kawashima Y, Omae T. Surgical management of infective endocarditis associated with cerebral complications; multicenter retrospective study in Japan. J Thorac Cardiovasc Surg 1995;110:1745–1755.
Hill EE, Herregods MC, Vanderschueren S, Claus P, Peetermans WE, Herijgers P. Outcome of patients requiring valve surgery during active infective endocarditis. Ann Thorac Surg 2008;85:1564–1569.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yamasaki, M., Watanabe, S., Abe, K. et al. Successful surgical treatment with mitral valve replacement and coronary embolectomy in a patient with active infective endocarditis complicated by multiple septic embolisms involving cerebral arteries and the right coronary artery. Gen Thorac Cardiovasc Surg 58, 471–476 (2010). https://doi.org/10.1007/s11748-009-0550-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-009-0550-x