
Abstract
Objective
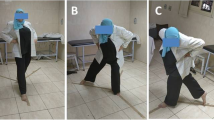
To evaluate the efficacy of Tuina (Chinese therapeutic massage) manipulation plus horse-riding squat exercise in treating knee osteoarthritis (KOA) and optimize the combining protocol.
Methods
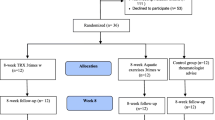
Based on a 2×2 factorial design, 120 eligible KOA patients were randomized into a manipulation group (group A1B2), a manipulation plus horse-riding squat group (group A1B1), a sitting knee-adjustment group (group A2B2 group), and a sitting knee-adjustment plus horse-riding squat group (group A2B1), with 30 cases in each group. The intervention was conducted three times a week, lasting for four weeks. The Western Ontario and McMaster Universities osteoarthritis index (WOMAC) was taken as the major measure for efficacy evaluation (including three component scores, pain, stiffness, and daily function, and total score).
Results
The three component scores (pain, stiffness, and daily function) and the total score of WOMAC showed significant differences after the intervention in the four groups (P<0.05). There were significant inter-group differences in the WOMAC stiffness score amongst the four groups after the intervention (P<0.05). In group A1B1, the step length, stride, walking speed, and knee joint flexion angle changed significantly after treatment (P<0.05). After the intervention, the step length changed significantly in group A1B2 (P<0.05), and the walking speed changed significantly in group A2B1 (P<0.05). There were no significant differences in the step length, stride, walking speed, or knee joint flexion angle among the four groups (P>0.05). The extensor peak torque at 180 °/s changed significantly in group A1B2 after treatment (P<0.05). Neither the intra-group nor the inter-group comparisons of the four groups revealed significant differences in the other isokinetic muscle strength parameters (P>0.05). The main effect of manipulation showed significant in affecting the WOMAC pain and total scores (P<0.05). The main effect of horse-riding squat exercise showed significant in affecting the WOMAC pain and stiffness scores (P<0.05).
Conclusion
The four treatment protocols all can improve the symptoms of KOA, for instance, relieving pain and stiffness, and enhancing daily function. Group A2B1 produces the most eminent effect in relieving joint stiffness. The main effects of both manipulation and horse-riding squat exercise are significant in reducing pain. Besides, the main effect of horse-riding squat exercise is significant in relieving joint stiffness.
【摘要】
目的
评价推拿手法结合马裆势练习治疗膝骨关节炎(KOA)的疗效, 以优化组合方案。
方法
采用2×2析因设计, 将120例符合纳入标准的KOA患者随机分为手法组(A1B2组), 手法结合马裆势组(A1B1组), 坐位调膝组(A2B2组)和坐位调膝结合马裆势组(A2B1组), 每组30例。患者每周干预3次, 持续4周。主要疗效评价指标为西安大略与麦克马斯特大学骨关节炎指数(WOMAC)评分(包括疼痛、僵硬、日常功能3项评分和总分), 次要疗效评价指标为步态分析(包括步长、步幅、步速和膝关节屈曲角度)和等速肌力测试(60 °/s和180 °/s角速度下的屈肌和伸肌峰力矩)。
结果
四组WOMAC疼痛、僵硬、日常功能3项评分和总分治疗前后组内差异均具有统计学意义(P<0.05)。四组治疗后WOMAC僵硬评分有统计学差异(P<0.05)。A1B1组治疗前后步长、步幅、步速及膝关节屈曲角度的差异有统计学意义(P<0.05); A1B2组治疗前后步长具有统计学差异(P<0.05), A2B1组治疗前后步速具有统计学差异(P<0.05)。四组步长、步幅、步速和膝关节屈 曲角度组间差异均无统计学意义(P>0.05)。A1B2组治疗前后180 °/s角速度伸肌峰力矩有统计学差异(P>0.05)。等速肌力 测试的其余指标四组组内及组间差异均无统计学意义(P>0.05)。手法主效应对于WOMAC疼痛评分及总分的改变有统 计学意义(P>0.05); 马裆势练习主效应对WOMAC疼痛和僵硬评分的改变具有统计学意义(P>0.05)。
结论
四种治疗方 案均可以改善KOA症状, 如缓解疼痛和僵硬, 增强日常功能。A2B1组关节僵硬减轻效果最佳。手法治疗和马裆势练习 在缓解疼痛方面都起主效应作用。马裆势练习在减轻关节僵硬方面起主效应作用。
Similar content being viewed by others

References
Arthroplasty Group, Chinese Orthopaedic Association, Chinese Medical Association. Guideline on the diagnosis and treatment of osteoarthritis. Zhonghua Guke Zazhi, 2018, 38(12): 705.
RUHDORFER A, WIRTH W, HITZL W, NEVITT M, ECKSTEIN F. Association of thigh muscle strength with knee symptoms and radiographic disease stage of osteoarthritis: data from the osteoarthritis initiative. Arthritis Care Res (Hoboken), 2014, 66(9): 1344–1353.
TANG X, WANG S, ZHAN S, NIU J, TAO K, ZHANG Y, LIN J. The prevalence of symptomatic knee osteoarthritis in China: results from the China Health and Retirement Longitudinal Study. Arthritis Rheumatol, 2016, 68(3): 648–653.
JEVSEVAR D S. Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg, 2013, 21(9): 571–576.
Hochberg M C, Altman R D, Brandt K D, Clark B M, Dieppe P A, Griffin M R, Moskowitz R W, Schnitzer T J. Guidelines for the medical management of osteoarthritis. Part I. Osteoarthritis of the hip. American College of Rheumatology. Arthritis Rheum, 1995, 38(11): 1541–1546.
YAN J T. Science of Tuina. Beijing: China Press of Traditional Chinese Medicine, 2017.
XU J, LI J S. Science of Tuina Qigong Exercise. Shanghai: Shanghai Scientific & Technical Publishers, 2011.
LIU M, SUN LH, LIU GE. Economic burden and economic risk of five major chronic diseases among Chinese urban residents. Beijing Daxue Xuebao (Yixue Ban), 2014, 46(5): 782–789.
WANG K, DONG X, LIN J H. The fees of patients with knee osteoarthritis. Zhonghua Yixue Zazhi, 2017, 97(1): 29–32.
SHI F, GU K, LU W, WENG W F, ZHU M Y, PENG Y Y, FU D B, ZHU J L, FU H. The evaluation on economic burden of arthritis in Shanghai. Zhongguo Weisheng Ziyuan, 2007, 10(2): 92–94.
GONG L, SUN W Q, ZHANG H, CHEN Z W, YAN J T. Professor YAN Jun-tao’s academic experience of Tuina on treating keen osteoarthritis based on theory of Jinjing. Shanghai Zhongyiyao Zazhi, 2016, 50(4): 1–3, 33.
YAN M, ZHANG B B, JIA H L. Briefly analysis on the clinical applying of 12 Jingjin. Zhongyi Xuebao, 2015, 30(8): 1150–1152.
FELSON D T, NIU J, GUERMAZI A, ROEMER F, ALIABADI P, CLANCY M, TORNER J, LEWIS C E, NEVITT M C. Correlation of the development of knee pain with enlarging bone marrow lesions on magnetic resonance imaging. Arthritis Rheum, 2007, 56(9): 2986–2992.
BARKER K, LAMB S E, TOYE F, JACKSON S, BARRINGTON S. Association between radiographic joint space narrowing, function, pain and muscle power in severe osteoarthritis of the knee. Clin Rehabil, 2004, 18(7): 793–800.
PENG H, ZHANG L, LIAN K, CHEN S. Advances in the mechanism and comprehensive treatment of chronic pain in knee osteoarthritis. Linchuang Waike Zazhi, 2016, 24(6): 476–478.
HUANG J, PENG Z L, ZHUO L S. Influence of Tuina plus function training on the cytokines in synovial fluid in knee osteoarthritis rabbits. Shizhen Guoyi Guoyao, 2009, 20(6): 1383–1384.
CRANE J D, OGBORN D I, CUPIDO C, MELOV S, HUBBARD A, BOURGEOIS JM, TARNOPOLSKY MA. Massage therapy attenuates inflammatory signaling after exercise-induced muscle damage. Sci Transl Med, 2012, 4(119): 119ra13.
YANG D H, WEI Y. Heat shock protein 70 mRNA expression in peripheral white blood cells after Taijiquan exercise. Zhongguo Zuzhi Gongcheng Yanjiu Yu Linchuang Kangfu, 2011, 15(41): 7787–7790.
JI B, ZHANG S N, JIN H Z, SHAO M X. Influence of the four-finger Tui-Pushing manipulation on the pain index and β-endorphin in patients with lumbar disc herniation. Jiangsu Zhongyiyao, 2007, 39(10): 57–58.
QU Y J, XUAN Z J, FENG J. Clinical research on the short-term efficacy of massaging quadriceps for knee osteoarthritis. J Acupunct Tuina Sci, 2016, 14(3): 216–219.
WANG K, SONG Y J, DONG W T, SONG M. Clinical observation on the treatment of knee osteoarthritis in early and middle stages by tendon massage. Shaanxi Zhongyiyao Daxue Xuebao, 2019, 42(3): 77–81.
WANG C, SCHMID C H, IVERSEN M D, HARVEY W F, FIELDING R A, DRIBAN J B, PRICE L L, WONG J B, REID K F, RONES R. Comparative effectiveness of Tai Chi versus physical therapy for knee osteoarthritis. Ann Intern Med, 2016, 165(2): 77–86.
ZHANG H, WU J P, YAN Z, CHEN C. Clinical observation of sitting knee-adjustment manipulation for patellofemoral arthropathy based on the real world. Guizhou Yiyao, 2019, 43(9): 1452–1454.
ZHU Q G, FANG M, GONG L, JIANG S Y, SUN W Q, LI J H, LI Y. Gait analysis of patients with knee osteoarthritis before and after Chinese massage treatment. J Tradit Chin Med, 2015, 35(4): 411–416.
GONG L, FANG M, YAN J T, SUN W Q, FAN Y Z. Clinical study of Tuina manipulation on flexors and extensors in patients with knee osteoarthritis. Zhongguo Zhongyi Gushang Zazhi, 2011, 19(2): 6–9.
Acknowledgments
This work was supported by National Natural Science Foundation of China (国家自然科学基金项目, No. 8197151584); Shanghai Sailing Program (上海市“科技创 新行动计划”启明星培育杨帆专项, No. 22YF1444300); Three-year Development Project for Traditional Chinese Medicine of Shanghai [上海市进一步加快中医药事业发 展三年行动计划, No. ZY(2018–2020)-ZWB-1001-FWB-08]; Project of Non-drug Therapy Clinical Research Center (非药物疗法临床研究中心项目); Project Within the Budget of Shanghai University of Traditional Chinese Medicine (上海中医药大学预算内项目, No. 2021LK091).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Co-first Authors
XING Hua, doctoral candidate, resident physician; SHEN Jiayun, master degree, resident physician
Conflict of Interest
There is no potential conflict of interest in this article.
Statement of Informed Consent
The protocol and informed consent were approved by the Medical Ethics Committee of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine (Approval No. 2015034). This trial was registered in Chinese Clinical Trial Registry (No. ChiCTR-INR-17011916). Informed consent was obtained from all individual participants.
Rights and permissions
About this article

Cite this article
Xing, H., Shen, J., Gong, L. et al. Protocol-optimizing study of combining Tuina and horse-riding squat exercise for knee osteoarthritis. J. Acupunct. Tuina. Sci. 20, 139–151 (2022). https://doi.org/10.1007/s11726-022-1305-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11726-022-1305-9
Keywords
- Tuina
- Massage
- Manual Therapies
- Physical and Breathing Exercises
- Horse-riding Squat Exercise
- Osteoarthritis, Knee
- Factorial Design