
Abstract
To reduce noise pollution and consequently stress during robot-assisted laparoscopic radical prostatectomy (RALP) the aim of our study was to evaluate the silent operation theatre optimisation system (SOTOS) in its effectiveness. In the operating room (OR) the noise level is between 80 and 85 decibel (dB). Noise corresponds to a major stress factor for surgical teams and especially surgeons. The use of the da Vinci surgical system entails an additional aspect of noise in the OR. The SOTOS surgical team used wired or wireless headphone/microphone combinations to communicate. We measured sound pressure levels in two different locations in the OR and the heart rate of every surgical team member as an indicator of the stress level. We further captured subjective acceptance of SOTOS as well as perioperative data such as surgical time. We prospectively randomised 32 RALP patients into two study arms. Sixteen surgeries were performed using SOTOS and 16 without (control). Overall, the mean sound pressure level in the SOTOS group was 3.6 dB lower compared to the control (p < 0.001). The highest sound pressure level measured was 96 dB in the control group. Mean heart rates were 81.3 beats/min for surgeons and 90.8 beats/min for circulating nurses. SOTOS had no statistically significant effect on mean heart rates of the operating team. Subjective acceptance of SOTO was high. Our prospective evaluation of SOTOS in RALP could show a significant noise reduction in the OR and a high acceptance by the surgical stuff.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the operating room (OR) the average noise level is between 80 and 85 decibel (dB) [1]. Usage of instruments and dropping of materials peak up levels to 108 dB [1]. These values are comparable with noise levels obtained nearby a highway or an airport [1]. General recommendations for noise levels at a regular work place environment are about 45 dB [2]. Noise corresponds to a major stress factor for surgical teams and especially surgeons [3]. Moorthy et al. showed a negative association between stress and surgical performance of laparoscopic tasks [4, 5]. Harmful effects of noise on surgeons are even more apparent in complex procedures [6]. Noise may negatively affect the surgeon’s efficiency and consequently the outcome of surgeries, and further potentially comprise mainly cardiovascular health risks for surgeons [7,8,9,10,11,12]. Several recent studies investigated the relation of noise pollution and health. According to Babisch et al., a high exposition to noise (60 dB) leads to a higher risk of high blood pressure [13]. First data implicate that noise causes high cortisone serum levels, which could lead to osteoporosis, diabetes mellitus and coronary heart disease [10, 14].
Several studies issue the use of music during surgery. Music in the OR potentially creates a better working environment for both, patient and the surgical team [15]. Moris et al. showed that patients under general anesthesia require less anesthetics while listening to music [16]. Siu et al. demonstrated better performance of surgeons while playing music during robotic laparoscopic operation practice tasks [6]. Ullmann et al. showed a subjective positive effect of music on the staff working in ORs [17]. On the other hand, Weddon et al. showed that music in the OR could interfere with team communication and could be recognized as a potential safety hazard [18]. So, the effect of music in the OR remains unclear.
During the last years, robot-assisted laparoscopic radical prostatectomy (RALP) was established as surgical gold standard for patients with localized prostate cancer (PCa) [19]. The use of the da Vinci surgical system entails an additional aspect of noise and challenging communication in the OR [20]. In addition to an elevated noise level, the fact that the surgeon is placed in a console distant to the actual surgical field and the assisting staff makes direct communication more difficult. Within this context, Hodge et al. demonstrated “noise pollution” in the OR through speech interference and unnecessary background noise [1].
With regard to the potential risks of noise especially on health of surgical teams, noise and information overload in high-tech environments like with a surgical robot and the positive influence of music Friedrich et al. developed the “Silent Operating Theatre Optimisation System (SOTOS©)” [21]. SOTOS© is a complex communication tool developed for the usage in the OR [21]. This technical solution allows the surgical team to communicate via headphones for noise reduction and microphones for interactive communication. The so-called “noise gate” opens the microphone for speech up to a certain noise level and closes it automatically. Additionally music can be played individually for each team member [21]. The music played is interrupted through speech. Additionally, ventilator alarms and alarms caused by the circulation monitoring are linked to the headphones of the anaesthesiologist.
The aim of our study was to evaluate SOTOS© in the setting of RALP. We hypothesized that SOTOS© would lead to significant noise reduction and consequently lower stress levels for the surgical team.
Materials and methods
Study cohort
All patients who underwent RALP had localized PCa. Between March and June 2017, we prospectively randomized 32 RALPs into two study arms. Sixteen surgeries were performed using SOTOS© and 16 without. The surgeries were performed in a standardized surgical technique [22]. For each patient age, initial PSA-value, Gleason-Score and D’Amico risk classification for PCa were available [23]. We further registered transrectal measured prostate volume, previous abdominal surgery, and perioperative data such as surgical time, nerve sparing [24], and difficult surgical conditions such as abdominal adhesions. Postoperative data included postoperative complications (i.e., bleeding, transfusion), surgical site infections or lymphocele development and length of hospital stay.
Exclusion criteria consisted of patient colonization with multi-resistant bacteria, planned open radical prostatectomy or surgeries performed by more than one surgeon. The study was approved by the local Ethics Committee of the University Medical Center Göttingen (ID 12/12/14).
SOTOS©
Setting and development was previously described by Friedrich et al. [21]. The communication system SOTOS© was installed in a standardized way for each surgery. Figure 1 shows the SOTOS© setup in the da Vinci OR. All participants were connected via the central SOTOS© control unit to ensure an unhindered communication. The surgical team used wired or wireless headphone/microphone combinations to communicate. The circulating nurses and scrub nurses used wireless headphones. The surgeon, the surgical assistant (Fig. 2) and the anaesthesiologist used a wired headphone combination. All critical alarms were connected to the headphone of the anaesthesiologist to guarantee the patient’s safety.

SOTOS© setup in the da Vinci operating room (*wired headphones, **wireless headphones, red diamond noise measurement spots)

Surgical assistant with SOTOS©—wired headphone communication
Noise level measurement
A calibrated sound level meter (DL-161S, Voltcraft, Germany) was used for noise level measurements. We measured the sound pressure levels at two locations in the OR. One measurement unit was placed in a distance of 1 m to the da Vinci console and the other measurement unit in a 1-m distance to the surgical field (Fig. 1). A measurement point was set every second. The sound pressure level was measured with weighting Filter A, used for environmental noise measurement. Furthermore, we defined four operation-relevant time points for specific noise level measurements in the OR: skin cut, da Vinci docking, bladder neck incision and da Vinci undocking. For further analyses we measured sound levels 10 min before and after these time points.
Stress level measurement
During surgery each team member was equipped with a 4-canal electrocardiogram (ECG) to evaluate heart rates. The heart rate can be used as an indirect indicator for the individual stress level [25]. Systematic analyses of ECG data were performed with CardioDay (2016, GE Healthcare, Chicago, IL, USA). We erased movement artefacts and extracted minimal, maximal and mean heart rate for each participant (i.e., surgeon, assistant, circulating nurse and scrub nurse). Caused by a very frequent change of staff in the anesthesiology department during surgeries in the study period, data quantity and quality obtained were too weak to include anesthesiologists in the current analysis.
Subjective acceptance of SOTOS© among the surgical team
Each participant of our study had to complete a questionnaire with general questions related to the SOTOS© technique. Each SOTOS© team member could only give one answer to each question.
Statistical analysis
We analyzed the impact of SOTOS© on sound pressure levels and heart rates. The mean sound pressure levels were captured during the whole surgery and the four operation-relevant time points between both study groups using the Wilcoxon rank sum test. For the comparison of the mean heart rates of both groups the t test was used. Differences between categorical variables in both groups were compared using the Chi-square test. All analyses were performed using Statistical Package for the Social Sciences (SPSS, Inc., Chicago, IL, version 25).
Results
Clinical, oncological and perioperative data
Clinical as well as oncological patient characteristics are displayed in Table 1. Mean age was 68.2 years (standard deviation ± 6.4 years). All patients had similar initial PSA-values, Gleason-Scores and D'Amico risk classifications. Transrectal measured prostate size was similar in both groups.
Perioperative parameters are shown in Table 2. The surgical time between SOTOS© and control group did not differ significantly (p = 0.43). Nerve Sparing was performed in 11 and 10 RALPs in the SOTOS© and control group, respectively. Difficult surgical conditions occurred similarly in both groups. Postoperative complications and length of hospital stay were comparable in both groups (Table 2).
Noise measurement
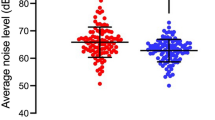
Noise measurement data are displayed in Fig. 3. Compared to the control the mean sound pressure level in the SOTOS© group captured during the whole surgery, was 3.6 dB lower (± 1.6 dB, p < 0.001). The highest sound pressure level peaks were 96 dB in the control group.

Mean sound pressure levels in dB during the whole surgery
Data measured at the four specific operation-relevant time points (skin cut, da Vinci docking, bladder neck incision and da Vinci undocking) are displayed in Fig. 4 and Table 3. The analyses revealed lower mean sound pressure levels at every situation (p < 0.001 respectively). Mean overall reduction of the sound pressure levels was 3.4 dB (between 3.0 and 3.8 dB) at these four situations.

Mean sound pressure levels in dB at four specific time points (i.e., skin cut, da Vinci docking, bladder neck incision and da Vinci undocking, ± 10 min)
Stress level measurement
We included 34 participants. The mean heart rates were captured by professional role (surgeon, assistant, circulating nurse and scrub nurses). Mean heart rates measured for the surgeon were 81.3 beats/min (± 7.1), for the assistant 87.7 beats/min (± 10.9), for the scrub nurse 86.9 beats/min (± 7.4) and circulating nurse 90.8 beats/min (± 7.4). SOTOS© had no statistically significant effect on mean heart rates of the operating team (p = 0.33). A subgroup analysis showed a significant reduction of the maximum heart rate for the circulating nurse in the SOTOS group (mean 111.6 ± 12 beats/min vs. 143.8 ± 35 beats/min (control group), p < 0.001; Fig. 5).

Maximal heart rate sorted by professional role in the OR for the SOTOS© and control group
Subjective acceptance of SOTOS© among the surgical team
For participants of the SOTOS©-Group the use of SOTOS© was….“extremely disturbing” in 1% (n = 1), “pretty disturbing” in 4% (n = 3)”, “little disturbing” in 10% (n = 7), “little supporting” in 6% (n = 4), “pretty supporting” in 56% (n = 40) and “extremely supporting” in 23% (n = 16) (Fig. 6). For surgeons, the question “I would like to use SOTOS© the whole time” was “pretty applicable” in one case (9%) and “extremely applicable” in 15 cases (93%).

Satisfaction of SOTOS© among the surgical team (i.e., surgeon, assistant, circulating nurse and scrub nurse), n = 71
Discussion
The aim of our study was to evaluate SOTOS© or noise and consequently stress reduction in a special communication setting like during RALP. Previous studies showed a negative effect of noise in the OR for the whole surgical team [3,4,5]. Friedrich et al. developed SOTOS© and were the first to show this new technical device to minimize noise exposure for cardiac surgery teams [21]. SOTOS© comprises not just noise reduction, but also shields disturbing environmental noise and offers immediate and direct voice information by the individual hearing. The music played further covers the residual noise level.
Our study presents data of the first use of SOTOS© during robotic-assisted laparoscopic surgery.
Our main finding was a significant noise reduction using SOTOS©. We demonstrated a maximal sound pressure level of 96 dB in the control group, which correlates to the massive noise levels in the OR during surgery. With SOTOS© noise reduction was recognized during the whole surgery and all specific key time points of the surgery. The extent of reduction during the whole surgery was 3.6 dB and between 3 and 3.8 dB at specific key time points. A decrease of sound pressure levels by 3 dB is equal to a halving of sound intensity.
For safe verbal communication we have to speak about 10 dB louder than the ambient noise. Since the environmental noise was the same in both groups with identical technical equipment, identical surgical procedure, the noise reduction must be mainly due to the quiet verbal communication within SOTOS. This should also have an effect on the indoor air hygiene, which could be shown in the working group of the heart surgeons in our university hospital. This is even more important in times of SARS2 pandemic problems.
Several studies exposed a negative influence of noise on health [8, 13, 26]. Additionally, Babisch et al. could demonstrate a correlation of traffic noise and cardiovascular health risk. They found a rising risk for ischemic cardiac disease over a sound pressure level of 65–70 dB, which we repeatedly captured during our study in the control group. Consequently, noise reduction with SOTOS© could possibly lead to a reduction of cardiac disease risk for the surgical team.
However, our study did not demonstrate a heart rate reduction as an indicator for stress using SOTOS in the OR. Heart rate alone cannot code safely for stress. Stress is a very broad field and requires several methods, some of them complex, to arrive a well-founded assessment. We can say that the evaluations of mean heart rates from this study do not give clear indications that SOTOS significantly changes stress in the team. Since further studies by extensive testing of psychologists showed that SOTOS is able to reduce stress, especially for surgeons, no further statement can be made with the limited data from this study [27].
One reason could be the different constitution and individual heart rates of the participants. Additionally, different influences like personal stress, constitution and non-predictable elements in day-to-day life of each participant could influence the heart rate. Another explanation could be a high rate of movement artefacts during the surgery, the reason why we could not analyze the heart rate variability, which could have better coded occupational stress [28]. Only the subgroup of the circulating nurse showed a significant reduction of maximal heart rates. This could be caused by the extensive movement of circulating nurses compared to the sterile surgical team and the surgeon at the console. SOTOS could cause less unnecessary physical activity by avoiding wrong information with a better communication using this system.
The median operating time was comparable to times published previously [29]. Surgeries in the SOTOS©-group were slightly shorter compared to the control (median 4 h and 6 min vs. 4 h and 20 min, p = 0.43). Although not statistically significant a shorter surgical time could indicate a better and direct communication between the surgical team. Hodge et al. presented results concerning communication problems caused by noise in the OR [1]. The shorter surgical time in the SOTOS©-group could also be an indicator for the positive effect of music use with SOTOS©.
Further, noise reduction using SOTOS© during RALP could possibly influence surgical performance and learning. Conrad et al. and Berguer et al. demonstrated a clear negative relation between noise in the OR and surgical motor performance and learning [9, 30]. Moorthy et al. showed less failure of operative tasks through noise reduction [5]. Within this context we could show a reduction of positive margins (not sign.) and a slightly shorter surgical time in the SOTOS©-group. This could be induced by either noise reduction, but also by music played during surgery. Siu et al. demonstrated a positive effect playing music during robotic-assisted laparoscopic procedures [6].
Using SOTOS© could probably lead to better communication by direct communication and muted environment. In 1956, Miller et al. described a limited short-term memory capacity of seven information or chunks [31]. This theory is controversial, but it shows the limited capacity of the central nerve system.
The general subjective acceptance of SOTOS© among the surgical team was good. For 85% of the participants SOTOS was supporting. This data strengthen the benefits of SOTOS© of leading to a better communication and interaction between the surgical team. Mainly the surgeons commented the system mostly positively and wanted to use the system the whole time. Further studies to investigate the reasons of the different acceptance of the system within the surgical team focusing on communication structure and technical benefits should be planned. Friedrich et al. could show that SOTOS© reduces questions and general communication during the surgery [21]. Bypassing the distance between surgeon and the rest of the team in the da Vinci OR could explain a subjective improvement for the surgeon and the team through SOTOS©.
Taken together reducing background noise and interferences using closed communication ways with the possibility to play music with SOTOS© could lead to higher concentration of surgeons, improve surgical tasks, enhance communication in the surgical team and finally have a distinct healthcare effect by noise and stress reduction.
Our study is the first to evaluate SOTOS© during RALP and to show its effect on noise reduction in this setting but focusing only on one surgery is a limitation of our study.
The missing effect on stress reduction through SOTOS must take influences such as personal stress and constitution into account. The measuring of stress is consequently challenging. The implementation of other methods such as skin impedance could be used for further investigations. However, also here personal influences might be unpredictable.
Another limitation of our study is the limited number of 32 surgeries. This limited number was caused by the high complexity of the measurements. Further studies with a larger number of surgeries, other surgical types like open surgery or transurethral procedures focusing on special aspects of the SOTOS© use may demonstrate further positive aspects of this tool and its impact on surgical outcomes.
Conclusion
Our prospective evaluation of SOTOS© in RALP could show a significant noise reduction in the OR and a high acceptance by the surgical stuff.
References
Hodge B, Thompson JF (1990) Noise pollution in the operating theatre. Lancet 335(8694):891–894
Cabrera IN, Lee MH (2000) Reducing noise pollution in the hospital setting by establishing a department of sound: a survey of recent research on the effects of noise and music in health care. Prev Med 30(4):339–345. https://doi.org/10.1006/pmed.2000.0638
Conrad C, Konuk Y, Werner P, Cao CG, Warshaw A, Rattner D, Jones DB, Gee D (2010) The effect of defined auditory conditions versus mental loading on the laparoscopic motor skill performance of experts. Surg Endosc 24(6):1347–1352. https://doi.org/10.1007/s00464-009-0772-0
Moorthy K, Munz Y, Dosis A, Bann S, Darzi A (2003) The effect of stress-inducing conditions on the performance of a laparoscopic task. Surg Endosc 17(9):1481–1484. https://doi.org/10.1007/s00464-002-9224-9
Moorthy K, Munz Y, Undre S, Darzi A (2004) Objective evaluation of the effect of noise on the performance of a complex laparoscopic task. Surgery 136(1):25–30. https://doi.org/10.1016/j.surg.2003.12.011(discussion 31)
Siu KC, Suh IH, Mukherjee M, Oleynikov D, Stergiou N (2010) The effect of music on robot-assisted laparoscopic surgical performance. Surg Innov 17(4):306–311. https://doi.org/10.1177/1553350610381087
Allen K, Blascovich J (1994) Effects of music on cardiovascular reactivity among surgeons. JAMA 272(11):882–884
Aydin Y, Kaltenbach M (2007) Noise perception, heart rate and blood pressure in relation to aircraft noise in the vicinity of the Frankfurt airport. Clin Res Cardiol 96(6):347–358. https://doi.org/10.1007/s00392-007-0507-y
Conrad C, Konuk Y, Werner PD, Cao CG, Warshaw AL, Rattner DW, Stangenberg L, Ott HC, Jones DB, Miller DL, Gee DW (2012) A quality improvement study on avoidable stressors and countermeasures affecting surgical motor performance and learning. Ann Surg 255(6):1190–1194. https://doi.org/10.1097/SLA.0b013e318250b332
Kirschbaum C, Hellhammer DH (1999) Noise and stress—salivary cortisol as a non-invasive measure of allostatic load. Noise Health 1(4):57–66
Sevdalis N, Healey AN, Vincent CA (2007) Distracting communications in the operating theatre. J Eval Clin Pract 13(3):390–394. https://doi.org/10.1111/j.1365-2753.2006.00712.x
Munzel T, Schmidt FP, Steven S, Herzog J, Daiber A, Sorensen M (2018) Environmental noise and the cardiovascular system. J Am Coll Cardiol 71(6):688–697. https://doi.org/10.1016/j.jacc.2017.12.015
Babisch W (2000) Traffic noise and cardiovascular disease: epidemiological review and synthesis. Noise Health 2(8):9–32
McEwen BS (1998) Protective and damaging effects of stress mediators. N Engl J Med 338(3):171–179. https://doi.org/10.1056/NEJM199801153380307
MacClelland DC (1979) Music in the operating room. AORN J 29(2):252–260
Moris DN, Linos D (2013) Music meets surgery: two sides to the art of “healing”. Surg Endosc 27(3):719–723. https://doi.org/10.1007/s00464-012-2525-8
Ullmann Y, Fodor L, Schwarzberg I, Carmi N, Ullmann A, Ramon Y (2008) The sounds of music in the operating room. Injury 39(5):592–597. https://doi.org/10.1016/j.injury.2006.06.021
Weldon SM, Korkiakangas T, Bezemer J, Kneebone R (2015) Music and communication in the operating theatre. J Adv Nurs 71(12):2763–2774. https://doi.org/10.1111/jan.12744
Trinh QD, Sammon J, Sun M, Ravi P, Ghani KR, Bianchi M, Jeong W, Shariat SF, Hansen J, Schmitges J, Jeldres C, Rogers CG, Peabody JO, Montorsi F, Menon M, Karakiewicz PI (2012) Perioperative outcomes of robot-assisted radical prostatectomy compared with open radical prostatectomy: results from the nationwide inpatient sample. Eur Urol 61(4):679–685. https://doi.org/10.1016/j.eururo.2011.12.027
Abbou CC, Hoznek A, Salomon L, Olsson LE, Lobontiu A, Saint F, Cicco A, Antiphon P, Chopin D (2001) Laparoscopic radical prostatectomy with a remote controlled robot. J Urol 165(6 Pt 1):1964–1966
Friedrich MG, Boos M, Pagel M, Thormann T, Berakdar A, Russo S, Tirilomis T (2017) New technical solution to minimise noise exposure for surgical staff: the ‘silent operating theatre optimisation system. BMJ Innov 3:196–205
Binder J, Kramer W (2001) Robotically-assisted laparoscopic radical prostatectomy. BJU Int 87(4):408–410
D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, Tomaszewski JE, Renshaw AA, Kaplan I, Beard CJ, Wein A (1998) Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 280(11):969–974
Asimakopoulos AD, Pereira Fraga CT, Annino F, Pasqualetti P, Calado AA, Mugnier C (2011) Randomized comparison between laparoscopic and robot-assisted nerve-sparing radical prostatectomy. J Sex Med 8(5):1503–1512. https://doi.org/10.1111/j.1743-6109.2011.02215.x
Dimitriev DA, Saperova EV (2015) Heart rate variability and blood pressure during mental stress. Ross Fiziol Zh Im I M Sechenova 101(1):98–107
Falk SA, Woods NF (1973) Hospital noise–levels and potential health hazards. N Engl J Med 289(15):774–781. https://doi.org/10.1056/NEJM197310112891504
Meyer-Lamp I, Boos M, Schugmann L, Leitsmann C, Trojan L, Friedrich M (2020) The silent operating theatre optimisation system for positive impact on surgical staff-members' stress, exhaustion, activity and concentration in urologic da Vinci® surgeries. A quasi-experimental field study. BMJ Innov (under review)
Jarvelin-Pasanen S, Sinikallio S, Tarvainen MP (2018) Heart rate variability and occupational stress-systematic review. Ind Health 56(6):500–511. https://doi.org/10.2486/indhealth.2017-0190
Kang J, Yoon KJ, Min BS, Hur H, Baik SH, Kim NK, Lee KY (2013) The impact of robotic surgery for mid and low rectal cancer: a case-matched analysis of a 3-arm comparison—open, laparoscopic, and robotic surgery. Ann Surg 257(1):95–101. https://doi.org/10.1097/SLA.0b013e3182686bbd
Berguer R, Smith WD, Chung YH (2001) Performing laparoscopic surgery is significantly more stressful for the surgeon than open surgery. Surg Endosc 15(10):1204–1207. https://doi.org/10.1007/s004640080030
Miller GA (1956) The magical number seven, plus or minus two: Some limits on our capacity for processing information. Psychol Rev 63(2):81
Funding
(Information that explains whether and by whom the research was supported): no funding was used in this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by CL, MF, AU and RW. The first draft of the manuscript was written by CL, MF, MB, RW, SA, and AU and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
No authors have conflicts of interest ore competing interest. Conrad Leitsmann, Annemarie Uhlig, I. Valentin Popeneciu, Margarete Boos, Sascha A. Ahyai, Marianne Schmid, Rolf Wachter, Lutz Trojan and Martin Friedrich declare that they have no conflict of interest.
Ethics approval
The study was performed as an individual diagnostic pathway per patient in consensus with the patient and was approved by the local Ethics Committee of the University Medical Center Goettingen (approval June 7, 2015). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Informed consent
The institutional review board of our institute approved this retrospective study, and the requirement to obtain informed consent was waived. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Leitsmann, C., Uhlig, A., Popeneciu, I.V. et al. The Silent Operation Theatre Optimisation System (SOTOS©) to reduce noise pollution during da Vinci robot-assisted laparoscopic radical prostatectomy. J Robotic Surg 15, 519–527 (2021). https://doi.org/10.1007/s11701-020-01135-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-020-01135-x