
Abstract
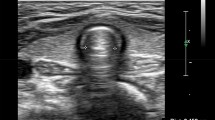
Robotic surgeries in the extreme Trendelenburg position can lead to changes in the airway dimensions. We conducted a prospective, observational trial to explore the use of ultrasound to quantify these changes in the airway dimensions and identify the factors associated with it. Fifty-two American society of Anaesthesiologists physical status I–II patients between 18 and 70 years of age of either sex scheduled to undergo robot assisted urological procedures in steep Trendelenburg position were enrolled. Anterior soft tissue thickness at the level of hyoid bone and vocal cords, tongue thickness, Malampatti grading and neck circumference were measured at predefined postoperative intervals in the immediate postoperative period, at 2-, 6- and 12-h period postoperatively. Linear stepwise regression analysis was done to explore the factors associated with change in anterior tissue thickness immediately after surgery. The mean difference (95%; CI) in the anterior soft tissue thickness in the immediate postoperative period at the level of hyoid was 0.023 (0.029–0.016) cm, p < 0.001 and at level of vocal cords was − 0.012 (− 0.017 to − 0.008) cm, p < 0.001 from the baseline. There was a significant increase in tongue thickness (0.002), Mallampati score (p = 0.002) and neck circumference (p < 0.001) in immediate postoperative period. The change in anterior tissue thickness at the level of hyoid was affected by total intraoperative fluids used (r = 0.602, p < 0.001), airway trauma (r = 0.275, p = 0.002) and duration of surgery (r = 0.243, p = 0.025). Significant changes in airway dimensions after robotic surgeries in Trendelenburg position persist till 2 h in the postoperative period which warrant vigilant monitoring for any airway compromise during this period.

Similar content being viewed by others

References
Hoshikawa Y, Tsutsumi N, Ohkoshi K et al (2014) The effect of steep Trendelenburg positioning on intraocular pressure and visual function during robotic-assisted radical prostatectomy. Br J Ophthalmol 98:305–308
Hamdy Awad H, Santilli S, Ohr M et al (2009) The effects of steep Trendelenburg positioning on intraocular pressure during robotic radical prostatectomy. Anesth Analg 109:473–478
Martínez-Salamanca JI, Romero Otero J (2007) Critical comparative analysis between open, laparoscopic and robotic radical prostatectomy: perioperative morbidity and oncological results (Part I). Arch Esp Urol 60:755–765
Phong SV, Koh LK (2007) Anaesthesia for robotic-assisted radical prostatectomy: considerations for laparoscopy in the Trendelenburg position. Anaesth Intensive Care 35:281–285
Goswami S, Nishanian E, Mets B (2010) Anesthesia for robotic surgery. In: Miller RD (ed) Miller’s anesthesia, 7th edn. Elsevier, Philadelphia, pp 2289–2395
Cook TM, Woodall N, Harper J, Benger J (2011) Fourth national audit project. Major complications of airway management in the UK: results of the fourth national audit project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: Intensive care and emergency departments. Br J Anaesth 106:632–642
Ezri T, Gewurtz G, Sessler DI et al (2003) Prediction of difficult laryngoscopy in obese patients by ultrasound quantification of anterior neck soft tissue. Anaesthesia 58:1111–1114
Singh M, Chin KJ, Chan VWS, Wong DT, Prasad GA, Yu E (2010) Use of sonography for airway assessment. J Ultrasound Med 29:79–85
Adhikari S, Zeger W, Schmier C et al (2011) Pilot study to determine the utility of point-of-care ultrasound in the assessment of difficult laryngoscopy. Acad Emerg Med 18:754–758
Wijeysundera DN, Sweitzer B (2015) Preoperative evaluation. In: Miller RD Miller’s anesthesia, 1092, 8th edn. Elsevier, Canada
Hauch MA, Datta S, Segal BS (1995) Maternal and fetal colloid osmotic pressure following fluid expansion during cesarean section. Crit Care Med 23:510–514
Lestar M, Gunnarsson L, Lagerstrand L, Wiklund P et al (2011) Hemodynamic perturbations during robot assisted laparoscopic radical prostatectomy in Trendelenburg position. Anesth Analg 113:1069–1075
Rewari V, Ramachandran R (2013) Prolonged steep Trendelenburg position: risk of postoperative upper airway obstruction. J Robot Surg 7:405–406
Menekse O, Ziya A, Hakan O et al (2014) Anesthetic considerations for robotic cystectomy: a prospective study. Rev Bras Anestesiol 64:109–115
Kilic OF, Börgers A, Köhne W et al (2015) Effects of steep Trendelenburg position for robotic-assisted prostatectomies on intra- and extrathoracic airways in patients with or without chronic obstructive pulmonary disease. Br J Anaesth 114:70–76
Komatsu R, Sengupta P, Wadhwa A et al (2007) Ultrasound quantification of anterior soft tissue thickness fails to predict difficult laryngoscopy in obese patients. Anaesth Intensive Care 35:32–37
Ushiroda J, Inoue S, Kirita T, Kawaguchi M (2014) A comparison of airway dimensions, measured by acoustic reflectometry and ultrasound before and after general anaesthesia. Anaesthesia 69:1355–1363
Wilson ME, John R (1990) Problems with the Mallampati sign. Anaesthesia 45:486–487
Bair AE, Caravelli R, Tyler K, Laurin EG (2010) Feasibility of the preoperative Mallampati airway assessement in emergency department patients. J Emerg Med 38:677–680
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Author Seran Reddy, Author Divya Jain, Author Kajal Jain, Author Komal Gandhi, Author Ravi Mohan, Author Mandeep Kang declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Reddy, S., Jain, D., Jain, K. et al. Changes in airway dimensions after robot assisted surgeries in steep Trendelenburg position. J Robotic Surg 13, 463–468 (2019). https://doi.org/10.1007/s11701-018-0869-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-018-0869-3