
Abstract
Background
The incidence of de novo gastroesophageal reflux disease (GERD) after LSG is substantial. However, an objective correlation with the structural gastric and EGJ changes has not been demonstrated yet. We aimed to prospectively evaluate the effects of laparoscopic sleeve gastrectomy (LSG) on the structure and function of the esophagogastric junction (EGJ) and stomach.
Methods
Investigations were performed before and after > 50% reduction in excess body weight (6–12 months after LSG). Subjects with GERD at baseline were excluded. Magnetic Resonance Imaging (MRI), high-resolution manometry (HRM), and ambulatory pH-impedance measurements were used to assess the structure and function of the EGJ and stomach before and after LSG.
Results
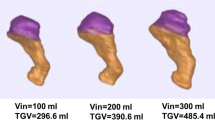
From 35 patients screened, 23 (66%) completed the study (age 36 ± 10 years, BMI 42 ± 5 kg/m2). Mean excess weight loss was 59 ± 18% after 7.1 ± 1.7-month follow-up. Esophageal acid exposure (2.4 (1.5–3.2) to 5.1 (2.8–7.3); p = 0.040 (normal < 4.0%)) and reflux events increased after surgery (57 ± 24 to 84 ± 38; p = 0.006 (normal < 80/day)). Esophageal motility was not altered by surgery; however, intrabdominal EGJ length and pressure were reduced (both p < 0.001); whereas the esophagogastric insertion angle (35° ± 11° to 51° ± 16°; p = 0.0004 (normal < 60°)) and esophageal opening diameter (16.9 ± 2.8 mm to 18.0 ± 3.7 mm; p = 0.029) were increased. The increase in reflux events correlated with changes in EGJ insertion angle (p = 0.010). Patients with > 80% reduction in gastric capacity (TGV) had the highest prevalence of symptomatic GERD.
Conclusion
LSG has multiple effects on the EGJ and stomach that facilitate reflux. In particular, EGJ disruption as indicated by increased (more obtuse) esophagogastric insertion angle and small gastric capacity were associated with the risk of GERD after LSG.
clinicaltrials.gov: NCT01980420



Similar content being viewed by others


References
Akkary E, Duffy A, Bell R. Deciphering the sleeve: technique, indications, efficacy, and safety of sleeve gastrectomy. Obes Surg. 2008;18(10):1323–9.
Colquitt JL, Picot J, Loveman E, et al. Surgery for obesity. Cochrane Database Syst Rev. 2009;15(2):CD003641.
Rebibo L, Dhahri A, Badaoui R, et al. Laparoscopic sleeve gastrectomy as day-case surgery (without overnight hospitalization). Surg Obes Relat Dis. 2015;11(2):335–42.
Hutter MM, Schirmer BD, Jones DB, et al. First report from the American College of Surgeons Bariatric Surgery Center Network: laparoscopic sleeve gastrectomy has morbidity and effectiveness positioned between the band and the bypass. Ann Surg. 2011;254(3):410–20. discussion 20-2
Peterli R, Wolnerhanssen BK, Peters T, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity: the SM-BOSS randomized clinical trial. JAMA. 2018;319(3):255–65.
Benaiges D, Goday A, Ramon JM, et al. Laparoscopic sleeve gastrectomy and laparoscopic gastric bypass are equally effective for reduction of cardiovascular risk in severely obese patients at one year of follow-up. Surg Obes Relat Dis. 2011;7(5):575–80.
Boza C, Gamboa C, Salinas J, et al. Laparoscopic roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy: a case-control study and 3 years of follow-up. Surg Obes Relat Dis. 2012;8(3):243–9.
Gagner M, Deitel M, Kalberer TL, et al. The second international consensus summit for sleeve gastrectomy, March 19-21, 2009. Surg Obes Relat Dis. 2009;5(4):476–85.
Boza C, Daroch D, Barros D, et al. Long-term outcomes of laparoscopic sleeve gastrectomy as a primary bariatric procedure. Surg Obes Relat Dis. 2014;10(6):1129–33.
Braghetto I, Csendes A, Korn O, et al. Gastroesophageal reflux disease after sleeve gastrectomy. Surg Laparosc Endosc Percutan Tech. 2010;20(3):148–53.
Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve gastrectomy for obesity. Ann Surg. 2010;252(2):319–24.
Rebecchi F, Allaix ME, Giaccone C, et al. Gastroesophageal reflux disease and laparoscopic sleeve gastrectomy: a physiopathologic evaluation. Ann Surg. 2014;260(5):909–14. discussion 14-5
Samakar K, McKenzie TJ, Tavakkoli A, et al. The effect of laparoscopic sleeve gastrectomy with concomitant hiatal hernia repair on gastroesophageal reflux disease in the morbidly obese. Obes Surg. 2016;26(1):61–6.
Sebastianelli L, Benois M, Vanbiervliet G, et al. Systematic endoscopy 5 years after sleeve gastrectomy results in a high rate of Barrett's esophagus: results of a multicenter study. Obes Surg. 2019;29(5):1462–9.
Genco A, Soricelli E, Casella G, et al. Gastroesophageal reflux disease and Barrett's esophagus after laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication. Surg Obes Relat Dis. 2017;13(4):568–74.
Felsenreich DM, Kefurt R, Schermann M, et al. Reflux, sleeve dilation, and Barrett's esophagus after laparoscopic sleeve gastrectomy: long-term follow-up. Obes Surg. 2017;27(12):3092–101.
Sohn S, Fischer J, Booth M. Adenocarcinoma of the gastro-oesophageal junction after sleeve gastrectomy: a case report. ANZ J Surg. 2017;87(10):E163–E4.
Santoro S. Technical aspects in sleeve gastrectomy. Obes Surg. 2007;17(11):1534–5.
Hamoui N, Anthone GJ, Kaufman HS, et al. Sleeve gastrectomy in the high-risk patient. Obes Surg. 2006;16(11):1445–9.
Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg. 2006;16(11):1450–6.
Klaus A, Weiss H. Is preoperative manometry in restrictive bariatric procedures necessary? Obes Surg. 2008;18(8):1039–42.
Laffin M, Chau J, Gill RS, et al. Sleeve gastrectomy and gastroesophageal reflux disease. J Obes. 2013;2013:741097.
Fujiwara Y, Nakagawa K, Tanaka T, et al. Relationship between gastroesophageal reflux and gastric emptying after distal gastrectomy. Am J Gastroenterol. 1996;91(1):75–9.
Hill LD, Kozarek RA, Kraemer SJ, et al. The gastroesophageal flap valve: in vitro and in vivo observations. Gastrointest Endosc. 1996;44(5):541–7.
Gyawali CP, Roman S, Bredenoord AJ, et al. Classification of esophageal motor findings in gastro-esophageal reflux disease: conclusions from an international consensus group. Neurogastroenterol Motil. 2017;29(12)
Jasper D, Freitas-Queiroz N, Hollenstein M, Misselwitz B, Layer P, Navarro-Rodriguez T, et al. Prolonged measurement improves the assessment of the barrier function of the esophago-gastric junction by high-resolution manometry. Neurogastroenterol Motil. 2017;29(2).
Schwizer W, Steingoetter A, Fox M. Magnetic resonance imaging for the assessment of gastrointestinal function. Scand J Gastroenterol. 2006;41(11):1245–60.
Curcic J, Fox M, Kaufman E, et al. Gastroesophageal junction: structure and function as assessed by using MR imaging. Radiology. 2010;257(1):115–24.
Curcic J, Roy S, Schwizer A, et al. Abnormal structure and function of the esophagogastric junction and proximal stomach in gastroesophageal reflux disease. Am J Gastroenterol. 2014;109(5):658–67.
Parker H, Hoad CL, Tucker E, et al. Gastric motor and sensory function in health assessed by magnetic resonance imaging: establishment of reference intervals for the Nottingham test meal in healthy subjects. Neurogastroenterol Motil. 2018;30(12):e13463.
NIH conference. Gastrointestinal surgery for severe obesity. Consensus development conference panel. Ann Intern Med 1991;115(12):956–961.
Fuchs KH, Babic B, Breithaupt W, et al. EAES recommendations for the management of gastroesophageal reflux disease. Surg Endosc. 2014;28(6):1753–73.
Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 2015;27(2):160–74.
Gyawali CP, Kahrilas PJ, Savarino E, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018;67(7):1351–62.
Parker HL, Tucker E, Hoad CL, et al. Development and validation of a large, modular test meal with liquid and solid components for assessment of gastric motor and sensory function by non-invasive imaging. Neurogastroenterol Motil. 2016;28(4):554–68.
Roy S, Fox MR, Curcic J, et al. The gastro-esophageal reflux barrier: biophysical analysis on 3D models of anatomy from magnetic resonance imaging. Neurogastroenterol Motil. 2012;24(7):616–25. e269
Fox M, Forgacs I. Gastro-oesophageal reflux disease. BMJ. 2006;332:88–93.
Jamieson JR, Stein HJ, DeMeester TR, et al. Ambulatory 24-h esophageal pH monitoring: normal values, optimal thresholds, specificity, sensitivity, and reproducibility. Am J Gastroenterol. 1992;87(9):1102–11.
Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999;45(2):172–80.
Curcic J, Schwizer A, Kaufman E, et al. Effects of baclofen on the functional anatomy of the oesophago-gastric junction and proximal stomach in healthy volunteers and patients with GERD assessed by magnetic resonance imaging and high-resolution manometry: a randomised controlled double-blind study. Aliment Pharmacol Ther. 2014;40(10):1230–40.
Korn O, Csendes A, Burdiles P, et al. Anatomic dilatation of the cardia and competence of the lower esophageal sphincter: a clinical and experimental study. J Gastrointest Surg. 2000;4(4):398–406.
Stein HJ, DeMeester TR, Peters JH, et al. Technique, indications, and clinical use of ambulatory 24-hour gastric pH monitoring in a surgical practice. Surgery. 1994;116(4):758–66. discussion 66-7
Braghetto I, Lanzarini E, Korn O, et al. Manometric changes of the lower esophageal sphincter after sleeve gastrectomy in obese patients. Obes Surg. 2010;20(3):357–62.
Yehoshua RT, Eidelman LA, Stein M, et al. Laparoscopic sleeve gastrectomy--volume and pressure assessment. Obes Surg. 2008;18(9):1083–8.
Mion F, Tolone S, Garros A, et al. High-resolution impedance manometry after sleeve gastrectomy: increased intragastric pressure and reflux are frequent events. Obes Surg. 2016;26(10):2449–56.
Coupaye M, Gorbatchef C, Calabrese D, et al. Gastroesophageal reflux after sleeve gastrectomy: a prospective mechanistic study. Obes Surg. 2018;28(3):838–45.
Acknowledgments
The authors would like to thank associate Professor Dr. Andreas Steingötter for his technical advice and support with acquisition and analysis of Magnetic Resonance Imaging.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Quero, G., Fiorillo, C., Dallemagne, B. et al. The Causes of Gastroesophageal Reflux after Laparoscopic Sleeve Gastrectomy: Quantitative Assessment of the Structure and Function of the Esophagogastric Junction by Magnetic Resonance Imaging and High-Resolution Manometry. OBES SURG 30, 2108–2117 (2020). https://doi.org/10.1007/s11695-020-04438-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-020-04438-y