
Abstract
Background
Enhanced Recovery After Surgery (ERAS) pathways have been shown to improve postoperative outcomes. However, its application in bariatric surgery is still limited. The aim of the study was to define the safety of ERAS in bariatric patients with regard to postoperative complications, length of hospital stay (LOS), and readmission rates within 30 days from surgery.
Methods
The effectiveness and safety of an ERAS protocol was prospectively investigated in morbidly obese patients who underwent bariatric surgery in a single-institute experience over a 2-year period.
Results
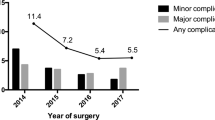
Between June 2016 and September 2018, a total of 89 laparoscopic sleeve gastrectomy (SG), 105 Roux-en-Y gastric bypass (RYGB), and 8 one-anastomosis gastric bypass (OAGB) were performed. Twenty patients (9.9%) were revisional cases. Mean (standard deviation, SD) BMI and age at time of surgery were 43.2 (± 6.2) kg/m2 and 46 (± 11.3) years, respectively. Median (range) surgical time was 118 (45–255) minutes. Overall postoperative complication rate was 7.4%, with 6 (3.0%) patients developing grade III–IV complications according to the Clavien-Dindo classification. Median (range) LOS was 2 (1–50) days, with mean (SD) LOS of 2.3 (± 3.6) days. Overall, 36.6% of patients were discharged by first postoperative day and 77.7% by second postoperative day. Readmission rate was 4.5%. No mortality was observed during the study period.
Conclusions
According to the results of the present study, ERAS in primary and revisional bariatric surgery is safe and feasible, with short LOS, low morbidity and readmission rates, and no mortality. A significant reduction of mean LOS was progressively noted over the study period.



Similar content being viewed by others


References
Hruby A, Hu FB. The epidemiology of obesity: a big picture. Pharmacoeconomics. 2015;33(7):673–89.
O’Brien PE. Bariatric surgery: mechanisms, indications and outcomes. J Gastroenterol Hepatol. 2010;25(8):1358–65.
Chang SH, Stoll CR, Song J, et al. The effectiveness and risks of bariatric surgery: an updated systematic review and meta-analysis, 2003-2012. JAMA Surg. 2014;149:275–87.
Arterburn DE, Courcoulas AP. Bariatric surgery for obesity and metabolic conditions in adults. BMJ. 2014;349:g3961.
Colquitt JL, Pickett K, Loveman E, et al. Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014;(8):CD003641.
Steele KE, Prokopowicz GP, Chang HY, et al. Risk of complications after bariatric surgery among individuals with and without type 2 diabetes mellitus. Surg Obes Relat Dis. 2012;8:305–30.
Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–17.
Varadhan KK, Neal KR, Dejong CH, et al. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. 2010;29(4):434–40.
Gustafsson UO, Scott MJ, Schwenk W, et al. Enhanced Recovery After Surgery (ERAS) Society for Perioperative Care, European Society for Clinical Nutrition and Metabolism (ESPEN), International Association for Surgical Metabolism and Nutrition (IASMEN). Guidelines for perioperative care in elective surgery: Enhanced Recovery After Surgery (ERAS(®)) society recommendation. World J Surg. 2013;37(2):259–84.
Bambgade OA, Adeogun BO, Abbas K. Fast-track laparoscopic gastric bypass surgery: outcomes and lessons from a bariatric surgery service in the United Kingdom. Obes Surg. 2012;22(3):398–402.
Lemanu DP, Singh PP, Berridge K, et al. Randomized clinical trial of enhanced recovery versus standard care after laparoscopic sleeve gastrectomy. Br J Surg. 2013;100:482–9.
Awad S, Carter S, Purkayastha S, Hakky S, Moorthy K, Cousins J, et al. Enhanced recovery after bariatric surgery (ERABS): clinical outcomes from a tertiary referral bariatric centre. Obes Surg 2014; 24:753–758.
Mannaerts GH, van Mil SR, Stepaniak PS, et al. Results of implementing an enhanced recovery after bariatric surgery (ERABS) protocol. Obes Surg. 2016;26(2):303–12.
Foschi D, De Luca M, Sarro G, Bernante P, Zappa MA, Moroni R, et al. Linee guida di buona pratica clinica nella selezione, nella preparazione, nel trattamento perioperatorio e a lungo termine del paziente obeso sottoposto a chirurgia bariatrica. Edizione 2016. Italian. Available from: https://www.sicob.org/00_materiali/linee_guida_2016.pdf
De Luca M, Angrisani L, Himpens J, et al. Indications for surgery for obesity and weight-related diseases: position statements from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes Surg. 2016;26(8):1659–96.
Thorell A, MacCormick AD, Awad S, et al. Guidelines for perioperative care in bariatric surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations. World J Surg. 2016;40(9):2065–83.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a color of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Małczak P, Pisarska M, Piotr M, et al. Enhanced recovery after bariatric surgery: systematic review and meta analysis. Obes Surg. 2017;27(1):226–35.
Blanchet MC, Gignoux B, Matussière Y, et al. Experience with an enhanced recovery after surgery (ERAS) program for bariatric surgery: comparison of MGB and LSG in 374 patients. Obes Surg. 2017;27(7):1896–900.
Barreca M, Renzi C, Tankel K, et al. Is there a role for enhanced recovery after laparoscopic bariatric surgery? Preliminary results from a specialist obesity treatment center. Surg Obes Rel Dis. 2016;12(1):119–26.
Hahl T, Peromaa-Haavisto P, Tarkiainen P, et al. Outcome of laparoscopic gastric bypass (LRYGB) with a program for enhanced recovery after surgery (ERAS). Obes Surg. 2016;26(3):505–11.
Dogan K, Kraaij L, Aarts EO, et al. Fast-track bariatric surgery improves perioperative care and logistics compared to conventional care. Obes Surg. 2015;25(1):28–35.
Geubbels N, Bruin SC, Acherman YI, et al. Fast track care for gastric bypass patients decreases length of stay without increasing complications in an unselected patient cohort. Obes Surg. 2014;24(3):390–6.
Author information
Authors and Affiliations
Contributions
CN: substantial contributions to the conception and design of the work, revising it critically for important intellectual content, final approval of the version to be published. He agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved. MT: substantial contributions to the conception and design of the work; acquisition, analysis, and interpretation of data for the work; drafting the work; and final approval of the version to be published. She agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved. DP: substantial contributions to the acquisition of data for the work, revising it critically for important intellectual content and final approval of the version to be published. He agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved. AB: substantial contributions to the interpretation of data for the work, revising it critically for important intellectual content, final approval of the version to be published. He agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Consent Statement
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nagliati, C., Troian, M., Pennisi, D. et al. Enhanced Recovery after Bariatric Surgery: 202 Consecutive Patients in an Italian Bariatric Center. OBES SURG 29, 3133–3141 (2019). https://doi.org/10.1007/s11695-019-03962-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-03962-w