
Abstract
Introduction
One-anastomosis-mini-gastric bypass (OAGB-MGB) is the second most popular gastric bypass procedure with remarkable weight loss results and comorbidity resolution rates. However, some concerns remain regarding its postoperative complications, including protein-calorie malnutrition (PCM). We hereby report our experience with patients who returned with severe PCM after OAGB-MGB.
Methods
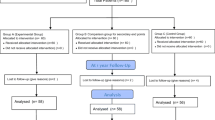
Patients with severe obesity presenting to our referral bariatric center underwent OAGB-MGB surgery using a 200-cm biliopancreatic limb (BPL) by a single surgical team at three university hospitals from March 2014 to February 2016.
Results
From 189 patients undergoing OAGB-MGB, seven patients (3.7%), all female, with a mean age of 46.4 ± 8.2 years and initial body mass index (BMI) of 44.2 ± 4.7 kg/m2, were readmitted for signs of PCM. Lower extremity edema, fatigue, excessive weight loss, hypoalbuminemia, anemia, and pancytopenia were the presenting symptoms and lab findings. Revisional surgery was performed at a mean 19 ± 9.7 months after OAGB-MGB after failure of supportive measures. The mean BMI at the time of revision was 22.5 ± 2.6 kg/m2 with an excess weight loss of 109.2 ± 22.1%. After revisional surgery, one patient developed profound liver failure and expired. Another patient developed severe steatohepatitis but ultimately recovered. In the remaining five, edema and fatigue completely resolved at 1 month and hypoalbuminemia and anemia normalized at 2 months.
Conclusion
A one-fits-all BPL length of 200 cm is increasingly being questioned as it may result in an inadequate absorptive area and PCM in a subset of patients with shorter total bowel lengths, potentially placing them in danger and depriving them of bariatric surgery benefits.
Similar content being viewed by others


References
Rutledge R. The mini-gastric bypass: experience with the first 1,274 cases. Obes Surg. 2001;11(3):276–80. https://doi.org/10.1381/096089201321336584.
Carbajo MA, Luque-de-Leon E, Jimenez JM, et al. Laparoscopic one-anastomosis gastric bypass: technique, results, and long-term follow-up in 1200 patients. Obes Surg. 2017;27(5):1153–67. https://doi.org/10.1007/s11695-016-2428-1.
Georgiadou D, Sergentanis TN, Nixon A, et al. Efficacy and safety of laparoscopic mini-gastric bypass. A systematic review. Surg Obes Relat Dis. 2014;10(5):984–91. https://doi.org/10.1016/j.soard.2014.02.009.
Musella M, Susa A, Manno E, et al. Complications following the mini/one anastomosis gastric bypass (MGB/OAGB): a multi-institutional survey on 2678 patients with a mid-term (5 years) follow-up. Obes Surg. 2017;27(11):2956–67. https://doi.org/10.1007/s11695-017-2726-2.
Schlottmann F, Nayyar A, Herbella FAM, et al. Preoperative evaluation in bariatric surgery. J Laparoendosc Adv Surg Tech A. 2018;28(8):925–9. https://doi.org/10.1089/lap.2018.0391.
Mahawar KK, Parmar C, Carr WRJ, et al. Impact of biliopancreatic limb length on severe protein-calorie malnutrition requiring revisional surgery after one anastomosis (mini) gastric bypass. J Minim Access Surg. 2018;14(1):37–43. https://doi.org/10.4103/jmas.JMAS_198_16.
Jammu GS, Sharma R. A 7-year clinical audit of 1107 cases comparing sleeve gastrectomy, Roux-En-Y gastric bypass, and mini-gastric bypass, to determine an effective and safe bariatric and metabolic procedure. Obes Surg. 2016;26(5):926–32. https://doi.org/10.1007/s11695-015-1869-2.
Ahuja A, Tantia O, Goyal G, et al. MGB-OAGB: effect of biliopancreatic limb length on nutritional deficiency, weight loss, and comorbidity resolution. Obes Surg. 2018;28(11):3439–45. https://doi.org/10.1007/s11695-018-3405-7.
Mahawar KK, Kumar P, Parmar C, et al. Small bowel limb lengths and Roux-en-Y gastric bypass: a systematic review. Obes Surg. 2016;26(3):660–71. https://doi.org/10.1007/s11695-016-2050-2.
Agha RA, Borrelli MR, Farwana R, et al. The PROCESS 2018 statement: Updating Consensus Preferred Reporting Of CasE Series in Surgery (PROCESS) guidelines. Int J Surg. 2018;60:279–82. https://doi.org/10.1016/j.ijsu.2018.10.031.
Barzin M, Hosseinpanah F, Motamedi MA, et al. Bariatric surgery for morbid obesity: Tehran Obesity Treatment Study (TOTS) rationale and study design. JMIR Res Protoc. 2016;5(1):e8. https://doi.org/10.2196/resprot.5214.
Motamedi MAK, Barzin M, Ebrahimi M, et al. Severe fatal protein malnutrition and liver failure in a morbidly obese patient after mini-gastric bypass surgery: case report. Int J Surg Case Rep. 2017;33:71–4. https://doi.org/10.1016/j.ijscr.2017.02.033.
Motamedi MAK, Rakhshani N, Khalaj A, et al. Biopsy-proven progressive fatty liver disease nine months post mini-gastric bypass surgery: a case study. Int J Surg Case Rep. 2017;39:168–71. https://doi.org/10.1016/j.ijscr.2017.07.062.
Mahawar KK, Himpens J, Shikora SA, et al. The first consensus statement on one anastomosis/mini-gastric bypass (OAGB/MGB) using a modified Delphi approach. Obes Surg. 2018;28(2):303–12. https://doi.org/10.1007/s11695-017-3070-2.
Nimeri A, Al Hadad M, Khoursheed M, et al. The peri-operative bariatric surgery care in the Middle East Region. Obes Surg. 2017;27(6):1543–7. https://doi.org/10.1007/s11695-016-2503-7.
Bruzzi M, Rau C, Voron T, et al. Single anastomosis or mini-gastric bypass: long-term results and quality of life after a 5-year follow-up. Surg Obes Relat Dis. 2015;11(2):321–6. https://doi.org/10.1016/j.soard.2014.09.004.
Lee WJ, Ser KH, Lee YC, et al. Laparoscopic Roux-en-Y vs. mini-gastric bypass for the treatment of morbid obesity: a 10-year experience. Obes Surg. 2012;22(12):1827–34. https://doi.org/10.1007/s11695-012-0726-9.
Mahawar KK, Borg CM, Kular KS, et al. Understanding objections to one anastomosis (mini) gastric bypass: a survey of 417 surgeons not performing this procedure. Obes Surg. 2017;27(9):2222–8. https://doi.org/10.1007/s11695-017-2663-0.
Nimeri A. Making sense of gastric/intestinal bypass surgeries: forget the name and remember the degree of restriction and malabsorption the surgeries provide. Surg Obes Relat Dis. 2017;13(4):716–9. https://doi.org/10.1016/j.soard.2017.01.001.
Hess DS. Limb measurements in duodenal switch. Obes Surg. 2003;13(6):966. https://doi.org/10.1381/096089203322618885.
Tacchino RM. Bowel length: measurement, predictors, and impact on bariatric and metabolic surgery. Surg Obes Relat Dis. 2015;11(2):328–34. https://doi.org/10.1016/j.soard.2014.09.016.
Mahawar KK. Gastric bypass is not a “restrictive and Malabsorptive” procedure. Obes Surg. 2016;26(9):2225–6. https://doi.org/10.1007/s11695-016-2270-5.
Lee WJ, Lee YC, Ser KH, et al. Revisional surgery for laparoscopic mini-gastric bypass. Surg Obes Relat Dis. 2011;7(4):486–91. https://doi.org/10.1016/j.soard.2010.10.012.
Acknowledgments
The author would like to thank Dr. M. Hassan K. Motamedi for his language edit of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This study was approved by the institutional review board (no. IR.SBMU.ENDOCRINE.REC 1397.0592018-05-08). Informed consent was obtained from all individual participants included in the study. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Khalaj, A., Kalantar Motamedi, M.A., Mousapour, P. et al. Protein-Calorie Malnutrition Requiring Revisional Surgery after One-Anastomosis-Mini-Gastric Bypass (OAGB-MGB): Case Series from the Tehran Obesity Treatment Study (TOTS). OBES SURG 29, 1714–1720 (2019). https://doi.org/10.1007/s11695-019-03741-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-03741-7