
Abstract
Background
The rate of surgical complications from bariatric procedures remains low despite an increase in volume. When serious complications occur, they are associated with an increased risk of mortality. The aim of this study is to determine if frail bariatric patients have an increased rate of Clavien level 4 and 5 complications. This study was conducted in participating hospitals in the National Surgical Quality Improvement Program (NSQIP).
Methods
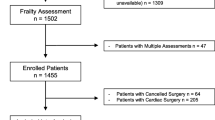
The NSQIP participant use files were used to identify 104,952 patients undergoing elective bariatric procedures from 2005 to 2012. A previously described modified frailty index (mFI) was calculated based on available NSQIP variables, with a higher index suggesting more frail patients. Postoperative adverse events were stratified to Clavien levels 4 and 5 utilizing a pre-existing mapping scheme.
Results
Overall, 1 % of patients undergoing elective bariatric surgery experienced Clavien level 4 complications, and 0.2 % experienced a Clavien level 5 complication (mortality). Univariate analysis demonstrated that frailty was significant for both Clavien level 4 and 5 complications (p < 0.001). The mean mFI for those with Clavien level 4 complications, 0.15, was significantly higher than those without Clavien 4 complications, 0.09 (p < 0.001). Those experiencing mortality had a mean mFI of 0.17 compared to a mean mFI of 0.09 in those without mortality (p < 0.001). Frailty retained the highest odds ratio for both Clavien 4 and 5 complications in multivariate analysis compared to American Society of Anesthesiologist (ASA) class, age, sex, body mass index (BMI), and procedure type.
Conclusions
Frailty may be used during patient selection to stratify bariatric surgery patients at high risk for critical care level complications.


Similar content being viewed by others


References
http://connect.asmbs.org/may-2014-bariatric-surgery-growth.html. Accessed 31 May 2014.
Fernandez AZ, DeMaria EJ, Tichansky DS, et al. Experience with over 3,000 open and laparoscopic bariatric procedures: multivariate analysis of factors related to leak and resultant mortality. Surg Endosc. 2004;18:193–7.
Birkmeyer N, Dimick J, Share D, et al. Hospital complication rates with bariatric surgery in Michigan. JAMA. 2010;304:435–42.
Fernandez AZ, DeMaria EJ, Tichansky DS, et al. Multivariate analysis of risk factors for death following gastric bypass for treatment of morbid obesity. Ann Surg. 2004;239:698–702.
Livingston EH, Huerta S, Arthur D, et al. Male gender is a predictor of morbidity and age a predictor of mortality for patients undergoing gastric bypass surgery. Ann Surg. 2002;236:576–82.
Padwal RS, Klarenback SW, Want X, et al. A simple prediction rule for all-cause mortality in a cohort eligible for bariatric surgery. JAMA. 2013;148:1109–15.
Flum DR, Salem L, Elrod JA, et al. Early mortality among medicare beneficiaries undergoing bariatric surgical procedures. JAMA. 2005;294:1903–8.
Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909–17.
Dorman R, Abraham A, Al-Refaie WB, et al. Bariatric surgery outcomes in the elderly: an ACS NSQIP study. J Gastrointest Surg. 2012;16:35–44.
Mitnitski A, Mogilner A, Rockwood K. Accumulation of deficits as a proxy measure of aging. Sci World J. 2001;1:323–36.
Velanovich V, Antoine H, Swartz A, et al. Accumulating deficits model of frailty and postoperative mortality and morbidity: its application to a national database. J Surg Res. 2013;183:104–10.
Abellan van Kan G, Rolland Y, Houles M, et al. The assessment of frailty in older adults. Clin Geriatr Med. 2010;26:275–86.
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–56.
Saxton A, Velanovich V. Preoperative frailty and quality of life as predictors of postoperative complications. Ann Surg. 2011;253:1223–9.
Obeid N, Azuh O, Reddy S, et al. Predictors of critical care-related complications in colectomy patients using the national surgical quality improvement program: exploring frailty and aggressive laparoscopic approaches. J Trauma Acute Care Surg. 2012;72:878–83.
Karam J, Tsiouris A, Shepard A, et al. Simplified frailty index to predict adverse outcomes and mortality in vascular surgery patients. Ann Vasc Surg. 2013;27:904–8.
Adams P, Ghanem T, Stachler R, et al. Frailty as a predictor of morbidity and mortality in inpatient head and neck surgery. JAMA Otolaryngol Head Neck Surg. 2013;139:783–9.
Hodari A, Hammoud ZT, Borgi JF, et al. Assessment of morbidity and mortality after esophagectomy using a modified frailty index. Ann Thorac Surg. 2013;96:1240–5.
Helling TS, Willoughby TL, Maxfield DM, et al. Determinants of the need for intensive care and prolonged mechanical ventilation in patients undergoing bariatric surgery. Obes Surg. 2004;14:1036–41.
Van den Broek RJ, Bruise MP, van Dielen FM, et al. Characteristics and outcome of patients admitted to the ICU following bariatric surgery. Obes Surg. 2009;19:560–4.
Hallowell PT, Stellato TA, Yao DA, et al. Should bariatric revisional surgery be avoided secondary to increased morbidity and mortality? Am J Surg. 2009;197:391–6.
Kermarrec N, Marmuse JP, Faivre J, et al. High mortality rate for patients requiring intensive care after surgical revision following bariatric surgery. Obes Surg. 2008;18:171–8.
Searle SD, Mitnitski A, Gahbauer EA, et al. A standard procedure for creating a frailty index. BMC Geriatr. 2008;8:24–33.
Dindo D, Demartines N, Clavien P. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Webb S, Rubinfeld I, Velanovich V, et al. Using National Surgical Quality Improvement Program (NSQIP) data for risk adjustment to compare Clavien 4 and 5 complications in open and laparoscopic colectomy. Surg Endosc. 2012;26:732–7.
Carlin AM, Zeni TM, English WJ, et al. The comparative effectiveness of sleeve gastrectomy, gastric bypass, and adjustable gastric banding procedures for the treatment of morbid obesity. Ann Surg. 2013;257:791–7.
Acknowledgements
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Conflict of Interest
Nina Kolbe DO, Arthur Carlin MD, Stephanie Bakey DO, Lisa Louwers MD, Mathilda Horst MD, and Ilan Rubinfeld MD have no conflicts of interest to disclose.
Ethical Approval
For this type of retrospective study, formal consent is not required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kolbe, N., Carlin, A.M., Bakey, S. et al. Assessing Risk of Critical Care Complications and Mortality in the Elective Bariatric Surgery Population Using a Modified Frailty Index. OBES SURG 25, 1401–1407 (2015). https://doi.org/10.1007/s11695-014-1532-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1532-3