
Abstract
Background
Severely obese type 2 diabetics who undergo Roux-en Y gastric bypass surgery have significant improvements in glycaemic control. Little work has been undertaken to establish the independent predictors of such resolution or to develop a predictive model. The aim of this study was to develop a mathematical model and establish independent predictors for the resolution of diabetes.
Methods
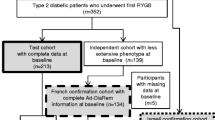
A consecutive sample of 130 severely obese type 2 diabetics who underwent gastric bypass surgery for weight loss from November 1997 to May 2007 with prospective pre-operative documentation of biochemical and clinical measurements was followed up over 12 months. Logistic discrimination analysis was undertaken to identify those variables with independent predictive value and to develop a predictive model for resolution of type 2 diabetes. Consecutive samples of 130 patients with body mass index (BMI) ≥ 35 with type 2 diabetes were selected. One hundred and twenty-seven patients completed the study with a sufficient data set. Patients were deemed unresolved if (1) diabetic medication was still required after surgery; (2) if fasting plasma glucose (FPG) remained >7 mmol/L; or (3) HbA1c remained >7%.
Results
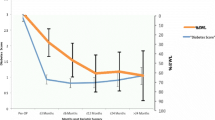
Resolution of diabetes was seen in 84%, while diabetes remained but was improved in 16% of patients. Resolution was rapid and sustained with 74% of those on medication before surgery being able to discontinue this by the time of discharge 6 days following surgery. Five pre-operative variables were found to have independent predictive value for resolution of diabetes, including BMI, HbA1c, FPG, hypertension and requirement for insulin. Two models have been proposed for prediction of diabetes resolution, each with 86% correct classification in this cohort of patients.
Conclusions
Type 2 diabetes resolves in a very high percentage of patients undergoing gastric bypass surgery for severe obesity. The key predictive variables include pre-operative BMI, HbA1c, FPG, the presence of hypertension and diabetic status.


Similar content being viewed by others

References
Wickremesekera K, Miller G, Naotunne TD, et al. Loss of insulin resistance after Roux-en-Y gastric bypass surgery: a time course study. Obes Surg. 2005;15(4):474–81.
Pories WJ, Swanson MS, MacDonald KG, et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg. 1995;222(3):339–50. discussion 350-332.
Kashyap SR, Daud S, Kelly KR, et al. Acute effects of gastric bypass versus gastric restrictive surgery on beta-cell function and insulinotropic hormones in severely obese patients with type 2 diabetes. Int J Obes (Lond). 2010;34(3):462–71.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–37.
Pories WJ, MacDonald Jr KG, Morgan EJ, et al. Surgical treatment of obesity and its effect on diabetes: 10-y follow-up. Am J Clin Nutr. 1992;55(2 Suppl):582S–5S.
Schauer PR, Burguera B, Ikramuddin S, et al. Effect of laparoscopic Roux-en Y gastric bypass on type 2 diabetes mellitus. Ann Surg. 2003;238(4):467–84. discussion 484–465.
Lee WJ, Ser KH, Chong K, et al. Laparoscopic sleeve gastrectomy for diabetes treatment in nonmorbidly obese patients: efficacy and change of insulin secretion. Surgery. 2010;147(5):664–9.
Fobi MA, Lee H. SILASTIC ring vertical banded gastric bypass for the treatment of obesity: two years of follow-up in 84 patients [corrected]. J Natl Med Assoc. 1994;86(2):125–8.
Fobi MA, Lee H. The surgical technique of the Fobi-Pouch operation for obesity (the transected silastic vertical gastric bypass). Obes Surg. 1998;8(3):283–8.
Witten IH, Frank E, editors. Data Mining: Practical Machine Learning Tools and Techniques. San Francisco, Ca, Morgan Kaufmann; 2005.
Cohen WW. Fast effective rule induction. Proceedings of the Twelfth International Conference of Machine Learning, Tahoe City, CA, Morgan Kaufmann; 1995.
Wild S, Roglic G, Green A, et al. Global prevalence of diabetes. Diab Care. 2004;27:1047–53.
Barr EL, Zimmet PZ, Welborn TA, et al. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: the Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation. 2007;116(2):151–7.
Standards of medical care in diabetes—2008. Diabetes Care. Jan 2008; 31 Suppl 1:S12–54.
Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA. 2004;291(3):335–42.
Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–59.
Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72.
Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360(2):129–39.
Rubino F, Forgione A, Cummings DE, et al. The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes. Ann Surg. 2006;244(5):741–9.
Laferrere B, Teixeira J, McGinty J, et al. Effect of weight loss by gastric bypass surgery versus hypocaloric diet on glucose and incretin levels in patients with type 2 diabetes. J Clin Endocrinol Metab. 2008;93(7):2479–85.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122(3):248–56. e245.
Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Clin Diabetes. 2009;27(1):4–16.
Cohen R, Pinheiro JS, Correa JL, et al. Laparoscopic Roux-en-Y gastric bypass for BMI < 35 kg/m(2): a tailored approach. Surg Obes Relat Dis. 2006;2(3):401–4. discussion 404.
DePaula AL, Macedo AL, Rassi N, et al. Laparoscopic treatment of type 2 diabetes mellitus for patients with a body mass index less than 35. Surg Endosc. 2008;22(3):706–16.
Scopinaro N, Papadia F, Marinari G, et al. Long-term control of type 2 diabetes mellitus and the other major components of the metabolic syndrome after biliopancreatic diversion in patients with BMI < 35 kg/m2. Obes Surg. 2007;17(2):185–92.
Sugerman HJ, Wolfe LG, Sica DA, et al. Diabetes and hypertension in severe obesity and effects of gastric bypass-induced weight loss. Ann Surg. 2003;237(6):751–6. discussion 757–758.
Adams TD, Gress RE, Smith SC, et al. Long-term mortality after gastric bypass surgery. N Engl J Med. 2007;357(8):753–61.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hayes, M.T., Hunt, L.A., Foo, J. et al. A Model for Predicting the Resolution of Type 2 Diabetes in Severely Obese Subjects Following Roux-en Y Gastric Bypass Surgery. OBES SURG 21, 910–916 (2011). https://doi.org/10.1007/s11695-011-0370-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-011-0370-9