
Abstract
Background
Different surgical techniques have been developed for the gastrojejunostomy (GJS) in laparoscopic Roux-en-Y gastric bypass (LRYGBP) with the anastomosis performed in a circular-stapled, linear-stapled, or totally hand-sewn way. No technique seems superior to the other as no consistent data on weight loss or complication rates were described.
Methods
A matched-pair study was conducted including a total of 150 patients, who underwent primary antegastric, antecolic LRYGBP between August 2003 and February 2007. Early weight loss and the incidence of GJS strictures or leaks and wound infections were compared between circular-stapled anastomosis (CSA) and linear-stapled anastomosis (LSA). Both groups were matched for age, sex, and body mass index.
Results
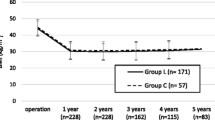
Excess weight loss at 3 months was slightly better with the CSA (p = 0.002) and comparable thereafter. Percentage of excess weight loss at 6, 12, and 24 months was 55.9 ± 17.5% vs. 51.2 ± 14.5%, 69.5 ± 20.9% vs. 71.4 ± 22.6%, and 70.8 ± 22.4% vs. 73.2 ± 23.4%, respectively (CSA vs. LSA). Strictures at the GJS were found only in the CSA group (n = 4), and leaks were found in one patient of the CSA group. More wound infections were observed in patients of the CSA group (ten vs. one).
Conclusions
CSA and LSA lead to comparable early weight loss in LRYGB. Thus, the technique is the surgeon's choice. In CSA, a higher incidence of GJS strictures and wound infections was observed. As weight regain following LRYGBP is commonly observed after at least 3 years, a longer follow-up is needed to compare the incidence of weight regain in circular- vs. linear-stapled GJS.

Similar content being viewed by others


References
Wittgrove AC, Clark GW, Tremblay LJ. Laparoscopic gastric bypass, Roux-en-Y: preliminary report of five cases. Obes Surg. 1994;4:353–7.
Korenkov M, Goh P, Yucel N, et al. Laparoscopic gastric bypass for morbid obesity with linear gastroenterostomy. Obes Surg. 2003;13:360–3.
Higa KD, Boone KB, Ho T, et al. Laparoscopic Roux-en-Y gastric bypass for morbid obesity: technique and preliminary results of our first 400 patients. Arch Surg. 2000;135:1029–33. discussion 33-4.
Wittgrove AC, Clark GW. Laparoscopic gastric bypass, Roux-en-Y- 500 patients: technique and results, with 3–60 month follow-up. Obes Surg. 2000;10:233–9.
Higa KD, Boone KB, Ho T. Complications of the laparoscopic Roux-en-Y gastric bypass: 1, 040 patients—what have we learned? Obes Surg. 2000;10:509–13.
Swartz DE, Gonzalez V, Felix EL. Anastomotic stenosis after Roux-en-Y gastric bypass: a rational approach to treatment. Surg Obes Relat Dis. 2006;2:632–6. discussion 7.
Ballesta-Lopez C, Poves I, Cabrera M, et al. Learning curve for laparoscopic Roux-en-Y gastric bypass with totally hand-sewn anastomosis: analysis of first 600 consecutive patients. Surg Endosc. 2005;19:519–24.
Carrodeguas L, Szomstein S, Zundel N, et al. Gastrojejunal anastomotic strictures following laparoscopic Roux-en-Y gastric bypass surgery: analysis of 1291 patients. Surg Obes Relat Dis. 2006;2:92–7.
Schwartz ML, Drew RL, Roiger RW, et al. Stenosis of the gastroenterostomy after laparoscopic gastric bypass. Obes Surg. 2004;14:484–91.
DeMaria EJ, Sugerman HJ, Kellum JM, et al. Results of 281 consecutive total laparoscopic Roux-en-Y gastric bypasses to treat morbid obesity. Ann Surg. 2002;235:640–5. discussion 5–7.
Abdel-Galil E, Sabry AA. Laparoscopic Roux-en-Y gastric bypass—evaluation of three different techniques. Obes Surg. 2002;12:639–42.
Gonzalez R, Lin E, Venkatesh KR, et al. Gastrojejunostomy during laparoscopic gastric bypass: analysis of 3 techniques. Arch Surg. 2003;138:181–4.
Schauer PR, Ikramuddin S, Gourash W, et al. Outcomes after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Ann Surg. 2000;232:515–29.
Papasavas PK, Caushaj PF, McCormick JT, et al. Laparoscopic management of complications following laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surg Endosc. 2003;17:610–4.
Shope TR, Cooney RN, McLeod J, et al. Early results after laparoscopic gastric bypass: EEA vs GIA stapled gastrojejunal anastomosis. Obes Surg. 2003;13:355–9.
Deitel M, Greenstein RJ. Recommendations for reporting weight loss. Obes Surg. 2003;13:159–60.
Deitel M, Gawdat K, Melissas J. Reporting weight loss 2007. Obes Surg. 2007;17:565–8.
Klingler A. Statistical methods in surgical research—a practical guide. Eur Surg. 2004;36:80–4.
Nguyen NT, Wolfe BM. Hypopharyngeal perforation during laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2000;10:64–7.
Scott DJ, Provost DA, Jones DB. Laparoscopic Roux-en-Y gastric bypass: transoral or transgastric anvil placement? Obes Surg. 2000;10:361–5.
Teixeira JA, Borao FJ, Thomas TA, et al. An alternative technique for creating the gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass: experience with 28 consecutive patients. Obes Surg. 2000;10:240–4.
Madan AK, Harper JL, Tichansky DS. Techniques of laparoscopic gastric bypass: on-line survey of American Society for Bariatric Surgery practicing surgeons. Surg Obes Relat Dis. 2007;4:166–72.
Gould JC, Garren M, Boll V, et al. The impact of circular stapler diameter on the incidence of gastrojejunostomy stenosis and weight loss following laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2006;20:1017–20.
Nguyen NT, Stevens CM, Wolfe BM. Incidence and outcome of anastomotic stricture after laparoscopic gastric bypass. J Gastrointest Surg. 2003;7:997–1003. discussion.
Cottam DR, Fisher B, Sridhar V, et al. The effect of stoma size on weight loss after laparoscopic gastric bypass surgery: results of a blinded randomized controlled trial. Obes Surg.; 2008.
Rice TW. Anastomotic stricture complicating esophagectomy. Thorac Surg Clin. 2006;16:63–73.
Barba CA, Butensky MS, Lorenzo M, et al. Endoscopic dilation of gastroesophageal anastomosis stricture after gastric bypass. Surg Endosc. 2003;17:416–20.
Ukleja A, Afonso BB, Pimentel R, et al. Outcome of endoscopic balloon dilation of strictures after laparoscopic gastric bypass. Surg Endosc. 2008;22:1746–50.
Lee JK, Van Dam J, Morton JM, et al. Endoscopy is accurate, safe, and effective in the assessment and management of complications following gastric bypass surgery. Am J Gastroenterol. 2009;104:575–82. quiz 83.
Csendes A, Burgos AM, Burdiles P. Incidence of anastomotic strictures after gastric bypass: a prospective consecutive routine endoscopic study 1 month and 17 months after surgery in 441 patients with morbid obesity. Obes Surg. 2009;19:269–73.
Christou NV, Look D, Maclean LD. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Ann Surg. 2006;244:734–40.
Z'Graggen K, Guweidhi A, Steffen R, et al. Severe recurrent hypoglycemia after gastric bypass surgery. Obes Surg. 2008;18:981–8.
Sczepaniak JP, Owens ML. Results of gastrojejunal anastomotic technique designed to reduce stricture. Surg Obes Relat Dis. 2009;5:77–80.
Chavarriaga LF, Cook MW, White B, et al. Transoral technique for gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass (LRYGBP) can accelerate learning curve and reduce cost. Obes Surg.; 2008.
Sekhar N, Torquati A, Lutfi R, et al. Endoscopic evaluation of the gastrojejunostomy in laparoscopic gastric bypass. A series of 340 patients without postoperative leak. Surg Endosc. 2006;20:199–201.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bohdjalian, A., Langer, F.B., Kranner, A. et al. Circular- vs. Linear-Stapled Gastrojejunostomy in Laparoscopic Roux-En-Y Gastric Bypass. OBES SURG 20, 440–446 (2010). https://doi.org/10.1007/s11695-009-9998-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-009-9998-0