
Abstract
Background
Obesity is an independent risk factor for cardiovascular disease, especially in its morbid form. Bariatric surgery is an effective therapeutic option for sustained weight loss. However, there is no consensus in these cases regarding the performance of functional tests for preoperative evaluations. The aim of the present study was to analyze clinical, electrocardiographic, and hemodynamic response variables using a conventional exercise test on individuals with morbid obesity in comparison to overweight individuals.
Methods
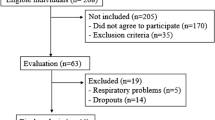
Six hundred seventeen cases were included. Group I had 290 patients with morbid obesity and group II had 327 overweight patients. All were submitted to a conventional treadmill exercise test. Classic positivity criteria were used.
Results
Both groups tolerated the test well. There was no statistically significant difference in terms of positivity of the test [ST segment abnormality or angor (P = 0.3863) or ST segment abnormality alone (P = 0.1000)]. The significantly higher values in the obese individuals were basal heart rate, basal systolic arterial pressure (SAP), maximum SAP, basal diastolic arterial pressure (DAP), maximum DAP, chronotropic deficit (P < 0.0001), and maximum rate–pressure product (P < 0.0421). The significantly lower values in the obese individuals were exercise time, maximum heart rate, and metabolic equivalents values (P < 0.0001).
Conclusion
Hemodynamic parameters were significantly different between the two groups. However, there were no differences in terms of ST segment abnormalities or effort-induced angina. The very low functional capacity and complex arrhythmia found in some obese individuals draws attention to the need for complementary investigation with the aim of diminishing the risk of postoperative heart complications.


Similar content being viewed by others

References
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. The evidence report. National Institutes of Health. Obes Res. 1998;6:51S–209S.
Poirier P, Giles TD, Bray GA, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006;113:898–918.
Hubert HB, Feinleib M, McNamara PM, et al. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983;67:968–77.
Messerli FH. Cardiopathy of obesity: a not-so-Victorian disease. N Engl J Med. 1986;314:378–80.
Björntorp P. Obesity. Lancet 1997;350:423–6.
Klein S, Burke LE, Bray GA, et al. American heart association council on nutrition, physical activity, and metabolism. Clinical implications of obesity with specific focus on cardiovascular disease: a statement for professionals from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation. Circulation 2004;110:2952–67.
Duflou J, Virmani R, Rabin I, et al. Sudden death as a result of heart disease in morbid obesity. Am Heart J. 1995;130:306–13.
de Divitiis O, Fazio S, Petitto M, et al. Obesity and cardiac function. Circulation 1981;64:477–82.
Iacobellis G, Ribaudo MC, Leto G, et al. Influence of excess fat on cardiac morphology and function: study in uncomplicated obesity. Obes Res. 2002;10:767–73.
Pascual M, Pascual DA, Soria F, et al. Effects of isolated obesity on systolic and diastolic left ventricular function. Heart 2003;89:1152–6.
Peterson LR, Waggoner AD, Schechtman KB, et al. Alterations in left ventricular structure and function in young healthy obese women: assessment by echocardiography and tissue Doppler imaging. J Am Coll Cardiol. 2004;43:1399–404.
Wong CY, O’Moore-Sullivan T, Leano R, et al. Association of subclinical right ventricular dysfunction with obesity. J Am Coll Cardiol. 2006;47:611–6.
Mitka M. Surgery for obesity: demand soars amid scientific, ethical questions. JAMA 2003;289:1761–2.
NIH Conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956–61.
McCullogh PA, Gallagher MJ, Dejong AT, et al. Cardiorespiratory fitness and short-term complications after bariatric surgery. Chest 2006;130:517–25.
Anonymous. Gastrointestinal surgery for severe obesity: National Institutes of the Health Consensus Development Conference Statement. Am J Clin Nutr. 1992;55:615S–619S.
Dolfing JG, Dubois EF, Wolffenbuttel BH, et al. Different cycle ergometer outcomes in severely obese men and women without documented cardiopulmonary morbidities before bariatric surgery. Chest 2005;128:256–62.
Serés L, López-Ayerbe J, Coll R, et al. Cardiopulmonary function and exercise capacity in patients with morbid obesity. Rev Esp Cardiol. 2003;56:594–600.
Serés L, Lopez-Ayerbe J, Coll R, et al. Increased exercise capacity after surgically induced weight loss in morbid obesity. Obesity 2006;14:273–9.
Karason K, Wallentin I, Larsson B, et al. Effects of obesity and weight loss on cardiac function and valvular performance. Obes Res. 1998;6:422–9.
Kanoupakis E, Michaloudis D, Fraidakis O, et al. Left ventricular function and cardiopulmonary performance following surgical treatment of morbid obesity. Obes Surg. 2001;11:552–8.
Gustafson AB, Farrell PA, Kalkhoff RK. Impaired plasma catecholamine response to submaximal treadmill exercise in obese women. Metabolism 1990;39:410–7.
Salvadori A, Fanari P, Mazza P, et al. Metabolic aspects and sympathetic effects in the obese subject undergoing exercise testing. Minerva Med. 1993;84:171–7.
Salvadori A, Fanari P, Mazza P, et al. Work capacity and cardiopulmonary adaptation of the obese subject during exercise testing. Chest 1992;101:674–9.
Salvadori A, Arreghini M, Bolla G, et al. Cardiovascular and adrenergic response to exercise in obese subjects. J Clin Basic Cardiol. 1999;2:229–36.
Salvadori A, Fanari P, Fontana M, et al. Oxygen uptake and cardiac performance in obese and normal subjects during exercise. Respiration 1999;66:25–33.
Gallagher MJ, Franklin BA, Ehrman JK, et al. Comparative impact of morbid obesity vs heart failure on cardiorespiratory fitness. Chest 2005;127:2197–203.
McNulty PH, Ettinger SM, Field JM, et al. Cardiac catheterization in morbidly obese patients. Catheteter Cardiovasc Interv. 2002;56:174–7.
Messerli FH, Ventura HO, Elizardi DJ, et al. Hypertension and sudden death. Increased ventricular ectopic activity in left ventricular hypertrophy. Am J Med. 1984;77:18–22.
Schunkert H. Obesity and target organ damage: the heart. Int J Obes. 2002;26:S15–20.
McHenry PL, Morris SN, Kavalier M, et al. Comparative study of exercise-induced ventricular arrhythmias in normal subjects and patients with documented coronary artery disease. Am J Cardiol. 1976;37:609–16.
Halpern SW, Mandel WJ. The significance of exercise-induced ventricular arrhythmias. Chest 1980;77:1–2.
Wolk R. Arrhythmogenic mechanisms in left ventricular hypertrophy. Europace 2000;2:216–23.
Frank S, Colliver JA, Frank A. The electrocardiogram in obesity: statistical analysis of 1,029 patients. J Am Coll Cardiol. 1986;7:295–9.
Russo V, Ammendola E, De Crescenzo I, et al. Effect of weight loss following bariatric surgery on myocardial dispersion of repolarization in morbidly obese patients. Obesity Surgery. 2007;17:857–65.
Lalani AP, Kanna B, John J, et al. Abnormal signal-averaged electrocardiogram (SAECG) in obesity. Obes Res. 2000;8:20–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fornitano, L.D., Godoy, M.F. Exercise Testing in Individuals with Morbid Obesity. OBES SURG 20, 583–588 (2010). https://doi.org/10.1007/s11695-008-9692-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9692-7