
Abstract
Background
Restrictive bariatric procedures are frequently considered for patients with morbid obesity, because the weight loss and reduction of comorbidities are good. An impact on gastroesophageal reflux disease (GERD), which is common in this population, may be anticipated. Converse results of GERD symptoms are reported for patients after adjustable gastric banding (AGB), sleeve gastrectomy (SG), and Roux-en-Y gastric bypass (RYGBP).
Methods
A literature search was performed and, with our personal experience, are summarized.
Results
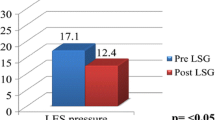
Esophageal manometry is a practical tool to identify functional disorders of the esophageal body and the lower esophageal sphincter (LES). For patients with weak esophageal body motility, AGB should not be considered as a therapeutic option because esophageal dilation, esophageal stasis, and consequent esophagitis often occur during long-term follow-up, and band deflation is inevitable. Stable body weight can therefore not be achieved in these patients. Low resting pressure of the LES may be a contraindication for SG, because taking away the angle of His further impairs the antireflux mechanism at the cardia. So far, RYGBP is an option for all morbidly obese patients regardless of the results of esophageal manometry.
Conclusion
Preoperative esophageal manometry is advised for restrictive procedures such as AGB and SG.


Similar content being viewed by others


References
Trus TL, Hunter JG. Minimally invasive surgery of the esophagus and stomach. Am J Surg. 1997;173:242–55.
Rippe JM. The obesity epidemic: challenges and opportunities. J Am Diet Assoc. 1998;98:5.
Fernandez AZ Jr, DeMaria EJ, Tichansky DS, et al. Experience with over 3000 open and laparoscopic bariatric procedures. Multivariate analysis of factors related to leak and resultant mortality. Surg Endosc. 2003;18:193–7.
SPECTRA Meinungsforschungsinstitut: Umfrage zum Thema Gewicht und Gewichtsreduktion. Interne Mitteilung der Firma Roche; 2000.
Kiefer I, Kunze M, Rieder A. Epidemiologie der Adipositas. J Ernährmed. 2001;1:17–9.
Hampel H, Abraham NS, El-Serag, et al. Meta analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005;143:199–211.
El-Serag HB, Graham DY, Satia JA, et al. Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am J Gastroenterol. 2005;100:1243–50.
Kitchin LI, Castell DO. Rationale and efficacy of conservative therapy for gastroesophageal reflux disease. Arch Intern Med. 1991;151:448–54.
Mercer CD, Rue C, Hanelin L, et al. Effect of obesity on esophageal transit. Am J Surg. 1985;149:177–81.
Wilson LJ, Ma W, Hirschowitz BI. Association of obesity with hiatal hernia and esophagitis. Am J Gastroenterol. 1999;94:2840–4.
Nilsson M, Johnsen R, Ye W, et al. Obesity and estrogen as risk factors for gastroesophageal reflux symptoms. JAMA. 2003;290:66–72.
Yang SS, Cheng KS, Lai YC, et al. Decreasing serum alpha-fetoprotein levels in predicting poor prognosis of acute hepatic failure in patients with chronic hepatitis B. J Gastroenterol. 2002;37:626–32.
Weiss HG, Nehoda H, Labeck B, et al. Treatment of morbid obesity with laparoscopic adjustable gastric banding affects esophageal motility. Am J Surg. 2000;180:479–82.
Labeck B, Nehoda H, Kuhberger-Peer R, et al. Adjustable gastric and esophagogastric banding. Is a pouch compulsory? Surg Endosc. 2001;15:1193–6.
Weiss HG, Nehoda H, Labeck B, et al. Adjustable gastric and esophagogastric banding: a randomized clinical trial. Obes Surg. 2002;12:573–8.
Klaus A, Gruber I, Wetscher G, et al. Prevalent esophageal body motility disorders underlie aggravation of GERD symptoms in morbidly obese patients following adjustable gastric banding. Arch Surg. 2006;141:247–51.
Klaus A, Raiser F, Swain JM, et al. Manometric components of the lower esophageal double hump. Dig Dis. 2000;18:172–7.
Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg. 2006;16:1450–6.
Melissas J, Koukouraki S, Askoxylakis J, et al. Sleeve gastrectomy: a restrictive procedure? Obes Surg. 2007;17:57–62.
Perry Y, Courcoulas AP, Fernando HC, et al. Laparoscopic Roux-en-Y gastric bypass for recalcitrant gastroesophageal reflux disease in morbidly obese patients. JSLS. 2004;8:19–23.
Bloomberg RD, Urbach DR. Laparoscopic Roux-en-Y gastric bypass for severe gastroesophageal reflux after vertical banded gastroplasty. Obes Surg. 2002;12:408–11.
Frezza EE, Ikramuddin S, Gourash W, et al. Symptomatic improvement in gastroesophageal reflux disease (GERD) following laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2002;16:1027–31.
Schauer P, Hamad G, Ikramuddin S. Surgical management of gastroesophageal reflux disease in obese patients. Semin Laparosc Surg. 2001;8:256–64.
Merrouche M, Sabaté JM, Jouet P, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly obese patients before and after bariatric surgery. Obes Surg. 2007;17:894–900.
Schauer PR, Ikramuddin S, Gourash W, et al. Outcomes after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Ann Surg. 2000;232:515–29.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Klaus, A., Weiss, H. Is Preoperative Manometry in Restrictive Bariatric Procedures Necessary?. OBES SURG 18, 1039–1042 (2008). https://doi.org/10.1007/s11695-007-9399-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9399-1