
Abstract
Background
Roux-en-Y gastric bypass (RYGBP) has been found to be the most efficient way to lose weight and maintain the weight loss in morbid obesity. However, with the formation of a new stomach and the modification of intestinal anatomy, there are significant changes on physiological properties of these organs that lead to nutrient deficiency, including calcium. The objectives of this study were to evaluate calcium intake, bone metabolism, and prevalence of metabolic bone disease in women subjected to RYGBP after 8 years.
Methods
Food frequency questionnaire and 3-day dietary recall, laboratory tests of bone metabolism and bone mineral density were accessed.
Results
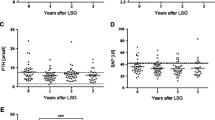
Calcium intake was below the recommendation in all women. Serum PTH and alkaline phosphatase were elevated, whereas vitamin D and urinary calcium were significantly lower. Also, a higher prevalence of metabolic bone disease than the one expected for the normal population at the same age was noted.
Conclusion
These data suggest that metabolic bone disease could be a complication of this type of surgery.


Similar content being viewed by others

References
Snow V, Barry P, Fitterman N, Qaseem A, Weiss K. Pharmacologic and surgical management of obesity in primare care: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2005;142:525–31.
Kushner, FR. Micronutrient deficiencies and bariatric surgery. Curr Opin Endocrinol Diabetes. 2006;13:405–11.
Shuster H, Vázquez J. Nutritional concern related to Roux-en-Y gastric bypass what every clinician needs to known. Crit Care Nurs Q. 2005;28(3):227–60.
Ott MT, Fanti P, Malluche HH, et al. Biochemical evidence of metabolic bone disease in women following Roux-in-Y gastric bypass for morbid obesity. Obes Surg. 1992;2:341–8.
Blake M, Fazio V, O’Brien P. Assessment of nutrient intake in association with weight loss after gastric restrictive procedures for morbid obesity. Aust NZ J Surg. 1991;61:195–9.
Coates OS, et al. Gastric bypass surgery for morbid obesity leads to an increase in bone turnover and a decrease in bone mass. J Clin Endocrinol Metab. 2004;89(3):1061–5.
Shaker JL, et al. Secondary hyperparathyroidism and osteopenia in women following gastric exclusion surgery for obesity. Osteoporos Int. 1991;1(3):177–81.
Goode LR, et al. Bone and gastric bypass surgery: effects of dietary calcium and vitamin D. Obes Res. 2004;12(1):40–7.
Fujoka K. Follow-up of nutritional and metabolic problems after bariatric surgery. Diabetes Care. 2005;28(2):481–4.
Langlois JA, Mussolino ME, Visser M, Looker AC, Harris T, Madans J. Weight loss from maximum body weight among middle-age and alder white women and the risk of hip fracture: the NHANES I epidemiologic follow-up study. Osteoporosis Int. 2001;12:763–8.
Bano G, et al. Reduced bone mineral density after surgical treatment for obesity. Int J Obes Relat Metab Disord. 1999;23(4):361–5.
Parfitt AM, Podenphant J, Villanueva AR, Frame B. Metabolic bone disease with and without osteomalacia afer intestinal bypass surgery: a bone histomorphometric study. Bone. 1985;6:211–20.
Compston JE, Vedi S, Gianetta W, Watson G, Civalleri D, Scopinaro N. Bone histomorphometry and vitamin D status after biliopancreatic bypass for morbid obesity. Gastroenterology. 1984;87:350–6.
Hey H, Lund B, Sorensen OH, Lund B. Delayed fracture healing following jejunoileal bypass surgery for obesity. Calcif Tissue Int. 1982;34:13–5.
Comision Europea. Informe sobre la osteoporosis en la comunidad Europea: Accion para la prevencion. Luxemburgo: Oficina de Publicationes Oficiales de las Comunidades Europeas, 1998. 116 ppt.
Montilla RHG, Aldrighi JM, Marucci MFN. Relação cálcio/proteína da dieta de mulheres no climatério. Rev Assoc Med Bras. 2004;50(1):52–4.
Galeazzi MAM, Domene SMA, Sichiere R. Estudo multicêntrico sobre o consumo alimentar. Cadernos de Debate—Revista Núcleo de Estudos e Pesquisas em Alimentação/UNICAMP. Ministério da Saúde; 1997. Volume Especial.
Slater GH, et al. Serum fat-soluble vitamin deficiency and abnormal calcium metabolism after malabsortive bariatric surgery. J Gastrointest Surg. 2004;8:48–55.
Lips P. Wich circulating level of 25-hydroxyvitamin D is appropriate? J Steroid Biochem Mol Biol. 2004;89–90:611–4.
de Prisco C, Levine SN. Metabolic bone disease after gastric bypass for morbid obesity. Am J Med Sci. 2005;329:57–61.
Goldner WS, et al. Severe metabolic bone disease as a long-term complication of obesity surgery. Obes Surg. 2002;12:685–92.
Diniz Mde F, Diniz MT, Sanches SR, Salgado PP, Valadão MM, Araújo FC, et al. Elevated serum parathormone after Roux-en-Y gastric bypass. Obes Surg. 2004 Oct;14(9):1222–6.
El-Kadre LJ, Rocha PR, de Almeida Tinoco AC, Tinoco RC. Calcium metabolism in pre- and postmenopausal morbidly obese women at baseline and after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2004 Sep;14(8):1062–6.
Bacha B, et al. Osteomalacia due to vitamin D depletion: a neglected consequence of intestinal malabsorpition. Am J Med. 2000;108:296–300.
Bell NH. Bone loss and gastric bypass surgery for morbid obesity. J Clin Endocrinol Metab. 2004;89:1059–60.
Tothill P, Avenell A. Erros in dual-energy X-ray absorptiometry of the lumbar spine owing to fat distribution and soft tissue thickness during wheight change. Br J Radiol. 1994;67:71–5.
Azevedo MNL, Alencar R, Baptista R, Pasqualette Ha, Carneiro RA, Vianna U. Densidade mineral óssea antes da menopausa. Rev Brás Reumatol. 1997;37(4):201–4.
Zanette E, et al. Avaliação do diagnóstico densitométrico de osteoporose / osteopenia conforme o sítio ósseo. Arquivos Brasileiros de Endocrinolgia & Metabologia. 2003;47(1).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Duran de Campos, C., Dalcanale, L., Pajecki, D. et al. Calcium Intake and Metabolic Bone Disease after Eight Years of Roux-en-Y Gastric Bypass. OBES SURG 18, 386–390 (2008). https://doi.org/10.1007/s11695-007-9393-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9393-7