
Abstract
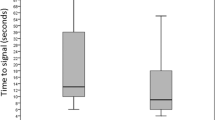
The esophagus is perfused directly by prominent arteries and may provide a more consistent tissue source for pulse oximetry. The goal of this study was to evaluate the sensitivity and accuracy of an esophageal pulse oximetry probe on patients during controlled hypoxemia in comparison to measurements obtained with conventional pulse oximetry (SpulseO2). Forty-five ASA I–II adult patients were included in this prospective observational study. Nellcor digital oximetric probes were placed on finger tips for SpulseO2 before anesthesia. After tracheal intubation, an esophageal probe was placed in the lower segment of the esophagus for esophageal oximetric monitoring (SoesO2). All patients were disconnected from the breathing circuit to establish a controlled hypoxemia, and were re-connected to the breathing circuit and ventilated with 100% oxygen immediately when SoesO2 dropped to 90%. Matched SoesO2 and SpulseO2 readings were recorded when SoesO2 measurements were at 100%, 95%, 90% and the lowest reading. The time for SoesO2 and SpulseO2 to drop from 100% to 95%, 90% and return to 100% was recorded. Oxygen saturation from arterial blood samples (SartO2) was also measured at each time point respectively. The linear correlation coefficient of the regression analysis between SartO2 and SoesO2 was 0.954. The mean ± 2SD of the difference was 0.3% ± 4.3% for SoesO2 vs. SartO2 and 6.8% ± 5.6% for SpulseO2 vs. SartO2 (P < 0.001). The 95% confidence interval for the absolute difference between SoesO2 and SartO2 was 0.3% to 0.7% and 6.2% to 7.4% between SpulseO2 and SartO2. The time to reach 90% saturation measured with SoesO2 was approximately 94 seconds earlier than the SpulseO2 (P < 0.001). In conclusion, SoesO2 is more accurate and enables earlier detection of hypoxemia when compared to conventional pulse oximetry during hypoxemia for patients undergoing general anesthesia.
Similar content being viewed by others

References
Pedersen T, Møller AM, Pedersen BD. Pulse oximetry for perioperative monitoring: systematic review of randomized, controlled trials. Anesth Analg 2003; 96(2): 426–431
Reich DL, Timcenko A, Bodian CA, Kraidin J, Hofman J, DePerio M, Konstadt SN, Kurki T, Eisenkraft JB. Predictors of pulse oximetry data failure. Anesthesiology 1996; 84(4): 859–864
Petterson MT, Begnoche VL, Graybeal JM. The effect of motion on pulse oximetry and its clinical significance. Anesth Analg 2007; 105(6 Suppl): S78–S84
Trivedi NS, Ghouri AF, Shah NK, Lai E, Barker SJ. Effects of motion, ambient light, and hypoperfusion on pulse oximeter function. J Clin Anesth 1997; 9(3): 179–183
Severinghaus JW, Kelleher JF. Recent developments in pulse oximetry. Anesthesiology 1992; 76(6): 1018–1038
Xue FS, Tong SY, Wang XL, Deng XM, An G. Study of the Optimal duration of preoxygenation in children. J Clin Anesth 1995;7(2): 93–96
Phillips JP, Kyriacou PA, Jones DP, Shelley KH, Langford RM. Pulse oximetry and photoplethysmographic waveform analysis of the esophagus and bowel. Curr Opin Anaesthesiol 2008; 21(6): 779–783
Phillips JP, Langford RM, Chang SH, Kyriacou PA, Jones DP. Photoplethysmographic measurements from the esophagus using a new fiber-optic reflectance sensor. J Biomed Opt 2011; 16(7): 077005
Margreiter J, Keller C, Brimacombe J. The feasibility of transesophageal echocardiograph-guided right and left ventricular oximetry in hemodynamically stable patients undergoing coronary artery bypass grafting. Anesth Analg 2002; 94(4): 794–798
Zhu ZQ, Wei W, Yang ZB, Liu AJ, Liu J. Transesophageal arterial oxygen saturation monitoring: an experimental study. J Sichuan Univ (Med Sci Ed) (Si Chuan Da Xue Xue Bao Yi Xue Ban) 2005; 36(1): 124–126 (in Chinese)
Phillips JP, Langford RM, Chang SH, Maney K, Kyriacou PA, Jones DP. Evaluation of a fiber-optic esophageal pulse oximeter. Conf Proc IEEE Eng Med Biol Soc 2009; 2009:1509–1512
Kyriacou PA, Jones DP, Langford RM, Petros AJ. A pilot study of neonatal and pediatric esophageal pulse oximetry. Anesth Analg 2008; 107(3): 905–908
Borum SE. The successful use of transesophageal pulse oximetry in a patient in whom peripheral pulse oximetry was unobtainable. Anesth Analg 1997; 85(3): 514–516
Vicenzi MN, Gombotz H, Krenn H, Dorn C, Rehak P. Transesophageal versus surface pulse oximetry in intensive care unit patients. Crit Care Med 2000; 28(7): 2268–2270
Kyriacou PA, Powell SL, Jones DP, Langford RM. Evaluation of oesophageal pulse oximetry in patients undergoing cardiothoracic surgery. Anaesthesia 2003; 58(5): 422–427
Xiong Q, Mu L, Wang L, Wei W. A pilot study of trans-esophageal aortic pulse oxygen saturation signals. J Biomed Eng ( ShengWu Yi Xue Gong Cheng Xue Za Zhi) 2010; 27(2): 266–269 (in Chinese)
Bland J, Altman D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1(8476): 307–310
Mannheimer PD. The light-tissue interaction of pulse oximetry. Anesth Analg 2007; 105(6 Suppl): S10–S17
Kyriacou PA, Powell S, Langford RM, Jones DP. Esophageal pulse oximetry utilizing reflectance photoplethysmography. IEEE Trans Biomed Eng 2002; 49(11): 1360–1368
Wei W, Zhu ZQ, Liu LX, Zuo YX, Gong M, Xue FS, Liu J. A pilot study of continuous transtracheal mixed venous oxygen saturation monitoring. Anesth Analg 2005; 101(2): 440–443
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, G., Zhu, Z., Liu, J. et al. Esophageal pulse oximetry is more accurate and detects hypoxemia earlier than conventional pulse oximetry during general anesthesia. Front. Med. 6, 406–410 (2012). https://doi.org/10.1007/s11684-012-0217-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11684-012-0217-3