
Abstract
The aim of the study was to find a descriptive rationale to quantify articular sided rotator cuff tears (PRCT) in the transversal and in the coronal plane leading to a two-dimensional description of the tear pattern.
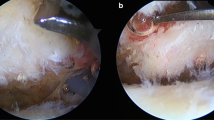
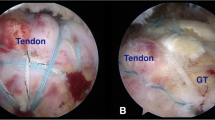
A total of 56 consecutive patients representing articular sided symptomatic PRCT diagnosed clinically and in MRI underwent standardized diagnostic arthroscopy. Intraarticular findings of the rotator cuff were classified according to Ellman and Synder. In addition the longitudinal tear was measured according to the length of the peeled off bony footprint in the paracoronal plane. The sagittal tear extension was defined as a tear of the lateral reflexion pulley (LRP) on the medial border of the supraspinatus tendon and/or a tear in the area of the crescent zone.
Statistically we observed a high correlation (r = 0.920; p < 0.0001) between the classification of Ellman and Snyder and only a slight correlation between the classification of Snyder as well as Ellman and this new classification.
Neither the classification according to Snyder nor the classification according to Ellman reproduce the extension of the partial thickness rotator cuff tears in the transversal and in the coronal plane related to its etiopathomorphology. This new classification takes the pathomorphology of the origin of partial thickness rotator cuff tears into account.
Zusammenfassung
Die Klassifikationen der RM-Partialrupturen nach Ellman sowie Snyder beschreiben die betroffene Sehnenfläche sowie die Läsionstiefe ohne die Ätiopathomorphologie der Rupturentstehung an der Sehneninsertion zu berücksichtigen. Ziel unserer prospektiven Studie war eine rationelle reproduzierbare Beschreibung zur Quantifizierung der artikularseitigen Rotatorenmanschettenpartialruptur (RMPR) zu entwickeln.
56 konsekutive Patienten mit klinischer und mittels MRT nachgewiesener artikularseitiger RMPR wurden standardisiert diagnostisch arthroskopiert. Die RMPR wurde intraoperativ nach Ellman und Snyder klassifiziert. Zusätzlich wurde das Ausmaß der RMPR zweidimensional gemessen. Die londitudinale Rupturausdehnung wurde anhand der Länge des freiliegenden knöchernen Footprints in der paracoronaren Ebene bestimmt. Die sagittale Rupturausdehnung in der transversalen Ebene wurde definiert als Ruptur des lateralen Pulley-Systems am medialen Supraspinatussehnenrand und / oder als Ruptur im Bereich der Crescent-Zone.
Arthroskopisch wiesen 71,4 % eine isolierte artikularseitige SSP-Ruptur und 28,6 % wiesen eine kombinierte artikularseitige SSP- und SCP-Ruptur auf.
62,5 % der Patienten mit artikularseitiger SSP-Ruptur hatten ein positives Cable-Sign.
In der transversalen Ebene wiesen Patienten mit artikularseitiger SSP-Ruptur in 26,8 % eine Ruptur des LCH, die sich in die SSP-Sehne fortsetzte (Zone A) auf. Bei 23,2 % fand sich eine artikularseitige SSP-Ruptur in der Crescent-Zone bei intaktem Rotatorenintervall (Zone B) und 50 % wiesen eine artikularseitige SSP-Ruptur mit Ausdehnung in Zone A und B auf.
In der paracoronaren Ebene fand sich bei 48,2 % eine Ausdehnung der artikularseitigen SSPRuptur in die Übergangszone von Knorpel zu Knochen (Typ 1), in 37,5 % eine Rupturausdehnung bis zur Mitte des Footprints (Typ 2) und in 14,2 % bis zum Tuberculum majus (Typ 3).
Statistisch wurde eine hohe Korrelation (Spearman's rho r = 0.920; p < 0.0001) zwischen der Klassifikation nach Ellman und nach Snyder beobachtet. Eine geringe Korrelation bestand (r = 0.342; p = 0.007) zwischen der Klassifikation nach Snyder und der Rupturausdehnung in der Übergangszone sowie zwischen der Klassifikation nach Ellman und der Rupturausdehnung and der Übergangszone (r = 0.376; p = 0.003).
Zwischen SSP-Rupturausdehnung bis zur Mitte des Footprints und der Klassifikation nach Ellman (r = 0.380; p = 0.003) sowie der Klassifikation nach Snyder (r = 0.326; p = 0.011) besteht ebenfalls nur eine geringe Korrelation.
Die Klasifikationen der artikularseitigen Supraspinatussehnenrupturen nach Snyder und nach Ellman reproduzieren nicht die Ausdehnung der Rotatorenmanschettenpartialruptur in der transversalen und in der coronaren Ebene ausgehend von der Sehneninsertion.
Similar content being viewed by others

Literatur
Andrews JR, Broussard TS, Carson WG (1985) Arthroscopy of the shoulder in the management of partial tears of the rotator cuff: a preliminary report. Arthroscopy 1:117–122
Bennett WF (2001) Subscapularis, medial, and lateral head coracohumeral ligament insertion anatomy. Arthroscopic appearance and incidence of “hidden” rotator interval lesions. Arthroscopy 17:173–180
Budoff JE, Nirschl RP, Ilahi OA, Rodin DM (2003) Internal impingement in the etiology of rotator cuff tendinosis revisited. Arthroscopy 19:810–814
Codman EA (1934) The Shoulder. Thomas Todd, Boston
Ellman H (1990) Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res 254:64–74
Gartsman GM (1995) Arthroscopic treatment of rotator cuff disease. J Shoulder Elbow Surg 4:228–241
Gerber C, Sebesta A (2000) Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: a preliminary report. J Shoulder Elbow Surg 9:483–490
Habermeyer P, Magosch P, Pritsch M, Scheibel MT, Lichtenberg S (2004) Anterosuperior impingement of the shoulder as a result of pulley lesions: a prospective arthroscopic study. J Shoulder Elbow Surg 13:5–12
Ide J, Maeda S, Takagi K (2005) Arthroscopic transtendon repair of partial-thickness articular-side tears of the rotator cuff: anatomical and clinical study. Am J Sports Med 33:1672–1679
Kuhn JE, Dunn WR, Ma B, Wright RW, Jones G, Spencer EE, Wolf B, Safran M, Spindler KP, McCarty E, Kelly B, Holloway B (2007) Interobserver Agreement in the Classification of Rotator Cuff Tears. Am J Sports Med 35(3):437–441
McConville OR, Iannotti JP (1999) Partial-thickness tears of the rotator cuff: evaluation and management. J Am Acad Orthop Surg 7:32–43
Nakajima T, Rokuuma N, Hamada K, Tomatsu T, Fukuda H (1994) Histologic and biomechanical characteristics of the supraspinatus tendon: Reference to rotator cuff tearing. J Shoulder Elbow Surg 3:79–87
Neer CS 2nd (1983) Impingement lesions. Clin Orthop Relat Res 173:70–77
Payne LZ, Altchek DW, Craig EV, Warren RF (1997) Arthroscopic treatment of partial rotator cuff tears in young athletes. A preliminary report. Am J Sports Med 25:299–305
Reilly P, Amis AA, Wallace AL, Emery RJ (2003) Supraspinatus tears: propagation and strain alteration. J Shoulder Elbow Surg 12:134–138
Reilly P, Macleod I, Macfarlane R, Windley J, Emery RJ (2006) Dead men and radiologists don't lie: a review of cadaveric and radiological studies of rotator cuff tear prevalence. Ann R Coll Surg Engl 88:116–121
Ruotolo C, Fow JE, Nottage WM (2004) The supraspinatus footprint: an anatomic study of the supraspinatus insertion. Arthroscopy 20:246–249
Sano H, Uhthoff HK, Backman DS, Brunet JA, Trudel G, Pham B, Ishii H (1998) Structural disorders at the insertion of the supraspinatus tendon. Relation to tensile strength. J Bone Joint Surg Br 80:720–725
Sano H, Wakabayashi I, Itoi E (2006) Stress distribution in the supraspinatus tendon with partial-thickness tears: an analysis using two-dimensional finite element model. J Shoulder Elbow Surg 15:100–105
Snyder SJ, Pachelli AF, Del Pizzo W, Friedman MJ, Ferkel RD, Pattee G (1991) Partial thickness rotator cuff tears: results of arthroscopic treatment. Arthroscopy 7:1–7
Walch G, Nove-Josserand L, Boileau P, Levigne C (1998) Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 7:100–108
Wolff AB, Sethi P, Sutton KM, Covey AS, Magit DP, Medvecky M (2006) Partialthickness rotator cuff tears. J Am Acad Orthop Surg 14:715–725
Author information
Authors and Affiliations
Corresponding author
Additional information
* Diese Arbeit wurde mit dem Best-Paper-Preis der DVSE ausgezeichnet.
Rights and permissions
About this article
Cite this article
Magosch, P., Krieter, C., Lichtenberg, S. et al. Eine neue arthroskopische Klassifikation der artikularseitigen Rotatorenmanschettenpartialruptur. Obere Extremität 3, 2–8 (2008). https://doi.org/10.1007/s11678-008-0071-8
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s11678-008-0071-8