
Abstract
Latissimus dorsi tendon transfer is an established method in the treatment of the nonrepairable rotator cuff tear. Originally, the muscle has to realize retroversion and internal rotation of the arm. After tendon transfer the function of the muscle is completely different from this – the muscle supports the elevation of the arm now. To take over the new function, patients need regulary for 9 to 12 months. In some studies this fact was controlled by surface electromyography (SEMG).
In our study we examined two groups of patients with a constant SEMG score 12 weeks after tendon transfer. One group received (a=30) common rehabilitation and the other patients (a=23) worked with SEMG-feedback therapy.
Muscle activity in patients with common rehabilitation (a=30) was not significantly increased in SEMG. But the latissimus dorsi in patients with SEMG (a=23) produced a high activity and a significant increase in the SEMG values. So far we found these results only in patients with normal therapy after 12 months.
In our opinion with the SEMG-feedback therapy it is possible to activate the latissimus dorsi in supporting the elevation of the arm in a more effective way and in a significantly shorter time.
Zusammenfassung
Die Latissimus-dorsi-Plastik (LDP) ist eine etablierte Methode zur Behandlung irreparabler Rotatorenmanschettenmassendefekte. Die Aufgabe des Muskels besteht originär in einer Abwärtsbewegung und Innenrotation des Armes. Nach der Transposition muss der Muskel eine völlig neue Funktion erlernen – er muss die Elevation unterstützen. Eine effiziente Übernahme der neuen Funktion (Rekrutierungszeitpunkt) dauert bei den meisten Patienten zwischen 9–12 Monaten und wurde in verschiedenen Studien mittels Oberflächenelektromyographie (OEMG) beschrieben.
In einer prospektiven Studie überprüften wir in einer Gruppe (n=30) nach üblicher Rehabilitation bzw. in einer Gruppe (n=23) mit Einsatz des OEMG-feedback-Trainings die Mittelwerte des Aktivitätsmusters im Oberflächen-EMG (OEMG) und den constant score 12 Wochen postoperativ.
Die Patienten mit konventioneller Nachbehandlung zeigten kaum erhöhte Aktivitätsmuster des Latissimus dorsi im OEMG. Demgegenüber fanden wir in der Gruppe mit OEMG-feedback-Training signifikant gestiegene OEMG-Werte, wie sie üblicherweise erst nach 9 bis 12 Monaten auftreten.
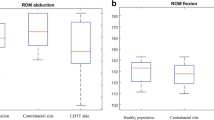
Diese Untersuchungsergebnisse widerspiegeln sich ebenfall im Constant Score beider Gruppen.
Unserer Meinung nach führt der postoperative Einsatz des OEMG-feedback-Trainings zu einer entscheidenden Verbesserung des Rekrutierungszeitpunktes des transferierten Muskels.
Similar content being viewed by others

Literatur
Aoki M, Okamura K, Fukushima S, Takahashi T, Ogino T (1996) Transfer of the latissimus dorsi for irreparable rotator cuff tears. J Bone Joint Surg Br 78(5):761–766
Alpert SW, Pink MM, Jobe FW, McMahon PJ, Mathiyakom W (2000) Electromyographic analysis of deltoid and rotator cuff function under varying loads and speeds. J Shoulder Elbow Surg 9:47–58
Bateman JE (1963) The diagnosis and treatment of ruptures of the rotator cuff. Surg Clin North Am 43:1523–1530
Constant CR (1991) Schulterfunktionsbeurteilung Orthopäde. 20(5):289–294 (in German)
Constant CR, Murley AH (1987) A clinical method of functional assessment of the shoulder. Clin Orthop 214:160–164
Constant CR (1986) Age related recovery of the shoulder function after injury. Thesis, University College, Cork, Ireland
Cram JR, Kaseman GS (1998) Instrumentation. In: Introduction to Surface Electromyography, Ch 3. ASPEN Publishers, Gaithersburg, Maryland, pp 43–78
Cram JR, Kaseman GS (1998) Electrodes and Site Selection Strategies. In: Introduction to Surface Electromyography, Ch 4. ASPEN Publishers, Gaithersburg, Maryland, pp 81–89
Cram JR, Kaseman GS (1998) Dynamic Assessment. In: Introduction to Surface Electromyography, Ch 8. ASPEN Publishers, Gaithersburg, Maryland, pp 153–166
Dumont CE, Gerber C (2000) Surgical technique of latissimus dorsi transfer for cuff deficiency. Techniques in Shoulder Elbow Surg 1(2):110–116
Fuchs B, Weishaupt D, Zanetti M, Hodler J, Gerber C (1998) Fatty degeneration of the muscles of the rotator cuff: assessment by computer tomography versus magnetic resonance imaging. J Shoulder Elbow Surg 8(6):599–605
Gansen HK, Irlenbusch U (2002) Die neuromuskuläre Insuffizienz der Rotatorenmanschette als Ursache des funktionellen Impingements – muskelbioptische Untersuchungen am Schultergelenk. Z Orthop 140:65–71 (in German)
Gartsman GM (1997) Massive, irreparable tears of the rotator cuff.Results of operative debridement and subacromial decompression. J Bone Joint Surg Am 79:715–721
Gattenlohner S, Schneider C, Thamer C, Klein R, Roggendorf W, Gohlke F, et al. (2002) Expression of fetal type acetylcholine receptor is restricted to type 1 muscle fibres in human neuromuscular disorders. Brain 125:1309–1319
Geiringer SR (2002) Elektromyographie – Atlas zur präzisen Muskellokalisation. München, Jena: Urban und Fischer, pp 36–49 (in German)
Gerber C, Maquieira G, Espinosa N (2006) Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears. J Bone Joint Surg Am 88(1):113–120
Gerber C (1992) Latissimus dorsi transfer for the treatment of irreparable tears of the rotator cuff. Clin Orthop Rel Res 275:152–160
Goutallier DPJM, Bernageau J, Lavau L, Voisin MC (1994) Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop 304:78–83
Habermeyer P, Lehmann L, Lichtenberg S (2000) Rotatorenmanschetten-Ruptur. Diagnostik und Therapie. Orthopäde 29:196–208 (in German)
Ianotti JP, Hennigan S, Herzog R, Kella S, Kelley M, Leggin B, Williams GR (2006) Latissimus dorsi tendon transfer for irreparable posteriosuperior rotator cuff tears. J Bone Joint Surg Am 88:342–348
Irlenbusch U, Bernsdorf M, Bracht M, Gansen HK, Lorenz U, Thiel J (2006) Latissimus dorsi transfer in case of irreparable rotator cuff tear – a longitudinal study in 52 patients over 50 months. J Shoulder Elbow Surg (in press)
Irlenbusch U, Bernsdorf M, Gansen HK, Lorenz U (2003) Latissimus-dorsi-Plastik zur Versorgung irreparabler Rotatorenmanschettenmassendefekte. Z Orthop 141:650–656 (in German)
Irlenbusch U, Gansen HK (2003) Muscle biopsy investigations on neuromuscular insufficiency of the rotator cuff – a contribution to the functional impingement of the shoulder joint. J Shoulder Elbow Surg 12:422–426
Katolik LI, Romeo AA, Cole BJ, Verma NN, Hyden JK, Bach BR (2005) Normalization in the constant score. J Shoulder Elbow Surg 14(3):279–285
Löhr JF (1999) Versorgung großer Rotatorenmanschettenrupturen. In: Imhoff AB, König U (eds) Schulterinstabilität – Rotatorenmanschette. Darmstadt: Steinkopf, pp 246–250 (in German)
Patte D (1990) Classification of rotator cuff lesions. Clin Orthop 254:81–86
Thomann SR, Dumont CE, Gerber C (2001) Die Verpflanzung des Musculus latissimus dorsi bei der Ruptur der Rotatorenmanschette. Operat Orthop Traumatol 3:159–169 (in German)
Thomazeau H (2001) Degenerative Veränderungen und Rotatorenmanschettendefekte. In: Radke S, Kenn W, Gohlke F (eds) MRT der Schulter. Orthopäde 30:484–491 (in German)
Warner JJP, Parsons IM (2001) Latissimus dorsi tendon transfer: A comparative analysis of primary and salvage reconstruction of massive, irreparable rotator cuff tears. J Shoulder Elbow Surg 10:514–521
Warner JJP (2001) Management of massive irreparable rotator cuff tears: the role of tendon transfer. Instr Course Lect 50:63–71
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bernsdorf, M., Born, S. & Irlenbusch, U. OEMG-Diagnostik und OEMG-biofeedback-Therapie nach Latissimus-dorsi-Plastik. Obere Extremität 2, 137–142 (2007). https://doi.org/10.1007/s11678-007-0047-0
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s11678-007-0047-0
Key words
- latissimus dorsi tendon transfer
- rotator cuff tear
- nonrepairable rotator cuff tear
- surface electromyography
- surface electromyography-feedback therapy