
Abstract
Summary
Femoral neck bone mineral density (BMD), age plus femoral neck BMD T score, and three externally generated fracture risk tools had similar accuracy to identify older men who developed osteoporotic fractures. Risk tools with femoral neck BMD performed better than those without BMD. The externally developed risk tools were poorly calibrated.
Introduction
We compared the performance of fracture risk assessment tools in older men, accounting for competing risks including mortality.
Methods
A comparative ROC curve analysis assessed the ability of the QFracture, FRAX® and Garvan fracture risk tools, and femoral neck bone mineral density (BMD) T score with or without age to identify incident fracture in community-dwelling men aged 65 years or older (N = 4994) without hip or clinical vertebral fracture or antifracture treatment at baseline.
Results
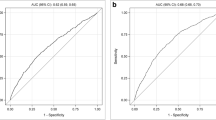
Among risk tools calculated with BMD, the discriminative ability to identify men with incident hip fracture was similar for FRAX (AUC 0.77, 95% CI 0.73, 0.81), the Garvan tool (AUC 0.78, 95% CI 0.74, 0.82), age plus femoral neck BMD T score (AUC 0.79, 95% CI 0.75, 0.83), and femoral neck BMD T score alone (AUC 0.76, 95% CI 0.72, 0.81). Among risk tools calculated without BMD, the discriminative ability to identify hip fracture was similar for QFracture (AUC 0.69, 95% CI 0.66, 0.73), FRAX (AUC 0.70, 95% CI 0.66, 0.73), and the Garvan tool (AUC 0.71, 95% CI 0.67, 0.74). Correlated ROC curve analyses revealed better diagnostic accuracy for risk scores calculated with BMD compared with QFracture (P < 0.0001). Calibration was good for the internally generated BMD T score predictor with or without age and poor for the externally developed risk tools.
Conclusion
In untreated older men without fragility fractures at baseline, an age plus femoral neck BMD T score classifier identified men with incident hip fracture as accurately as more complicated fracture risk scores.

Similar content being viewed by others

Change history
07 November 2017
Owing to an oversight by the authors, the acknowledgments were incomplete.
22 February 2023
A Correction to this paper has been published: https://doi.org/10.1007/s11657-023-01223-z
References
Moyer VA (2011) Screening for osteoporosis: U.S. preventive services task force recommendation statement. Ann Intern Med 154(5):356–364. https://doi.org/10.1059/0003-4819-154-5-201103010-00307
Zhou J, Wang T, Zhao X, Miller DR, Zhai S (2016) Comparative efficacy of bisphosphonates to prevent fracture in men with osteoporosis: a systematic review with network meta-analyses. Rheumatol Ther 3(1):117–128. https://doi.org/10.1007/s40744-016-0030-6
Barnard K, Lakey WC, Batch BC, Chiswell K, Tasneem A, Green JB (2016) Recent clinical trials in osteoporosis: a firm foundation or falling short? PLoS One 11(5):e0156068. https://doi.org/10.1371/journal.pone.0156068
Shawa H, Favela E, Diaz J (2011) Knowledge of osteoporosis among men in the primary care setting. South Med J 104(8):584–588. https://doi.org/10.1097/SMJ.0b013e3182241da1
Jain S, Bilori B, Gupta A, Spanos P, Singh M (2016) Are men at high risk for osteoporosis underscreened? A quality improvement project. Perm J 20(1):60–64. https://doi.org/10.7812/TPP/14-190
Centers for Medicare & Medicaid Services. (2017) Medicare.gov: the Official U.S. Government Site for Medicare. Your Medicare Coverage: bone mass measurement (bone density). https://www.medicare.gov/coverage/bone-density.html. Accessed 12 July 2017
Damji AN, Bies K, Alibhai SM, Jones JM (2015) Bone health management in men undergoing ADT: examining enablers and barriers to care. Osteoporos Int 26(3):951–959. https://doi.org/10.1007/s00198-014-2997-6
Kanis J, Johnell O, Oden A, Johansson H, McCloskey E (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19:385–397
Nguyen ND, Frost SA, Center JR, Eisman JA, Nguyen TV (2007) Development of a nomogram for individualizing hip fracture risk in men and women. Osteoporos Int 18(8):1109–1117. https://doi.org/10.1007/s00198-007-0362-8
Hippisley-Cox J, Coupland C (2009) Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ 339:b4229. https://doi.org/10.1136/bmj.b4229
Leslie WD, Lix LM (2014) Comparison between various fracture risk assessment tools. Osteoporos Int 25(1):1–21. https://doi.org/10.1007/s00198-013-2409-3
Marques A, Ferreira RJ, Santos E, Loza E, Carmona L, da Silva JA (2015) The accuracy of osteoporotic fracture risk prediction tools: a systematic review and meta-analysis. Ann Rheum Dis 74(11):1958–1967. https://doi.org/10.1136/annrheumdis-2015-207907
Kanis JA, Oden A, Johansson H, Borgstrom F, Strom O, McCloskey E (2009) FRAX and its applications to clinical practice. Bone 44(5):734–743. https://doi.org/10.1016/j.bone.2009.01.373
World Health Organization Collaborating Centre for Metabolic Bone Diseases. (2017) FRAX: WHO Fracture Risk Assessment Tool [Internet]. University of Sheffield, Sheffield, UK. Available from http://www.shef.ac.uk/FRAX. Accessed 12 September 2017
Nguyen ND, Frost SA, Center JR, Eisman JA, Nguyen TV (2008) Development of prognostic nomograms for individualizing 5-year and 10-year fracture risks. Osteoporosis International: a Journal Established as Result of Cooperation Between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA 19(10):1431–1444. https://doi.org/10.1007/s00198-008-0588-0
Collins GS, Mallett S, Altman DG (2011) Predicting risk of osteoporotic and hip fracture in the United Kingdom: prospective independent and external validation of QFractureScores. BMJ 342:d3651. https://doi.org/10.1136/bmj.d3651
Dagan N, Cohen-Stavi C, Leventer-Roberts M, Balicer RD (2017) External validation and comparison of three prediction tools for risk of osteoporotic fractures using data from population based electronic health records: retrospective cohort study. BMJ 356:i6755. https://doi.org/10.1136/bmj.i6755
Ensrud KE, Lui LY, Taylor BC, Schousboe JT, Donaldson MG, Fink HA, Cauley JA, Hillier TA, Browner WS, Cummings SR (2009) A comparison of prediction models for fractures in older women: is more better? Arch Intern Med 169(22):2087–2094. https://doi.org/10.1001/archinternmed.2009.404
Orwoll E, Blank JB, Barrett-Connor E, Cauley J, Cummings S, Ensrud K, Lewis C, Cawthon PM, Marcus R, Marshall LM, McGowan J, Phipps K, Sherman S, Stefanick ML, Stone K (2005) Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study—a large observational study of the determinants of fracture in older men. Contemp Clin Trials 26(5):569–585. https://doi.org/10.1016/j.cct.2005.05.006
Blank JB, Cawthon PM, Carrion-Petersen ML, Harper L, Johnson JP, Mitson E, Delay RR (2005) Overview of recruitment for the osteoporotic fractures in men study (MrOS). Contemporary Clinical Trials 26(5):557–568. https://doi.org/10.1016/j.cct.2005.05.005
World Health Organization. Assessment of osteoporotic fracture risk and its role in screening for postmenopausal osteoporosis. WHO Technical report series no. 843. Geneva: World Health Organization 1994
Hernlund E, Svedbom A, Ivergard M, Compston J, Cooper C, Stenmark J, McCloskey EV, Jonsson B, Kanis JA (2013) Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 8(1–2):136. https://doi.org/10.1007/s11657-013-0136-1
Watts NB, Leslie WD, Foldes AJ, Miller PD (2013) 2013 International Society for Clinical Densitometry Position Development Conference: task force on normative databases. Journal of clinical densitometry : the official journal of the International Society for Clinical Densitometry 16(4):472–481. https://doi.org/10.1016/j.jocd.2013.08.001
Looker A, Wahner H, Dunn W, Calvo M, Harris T, Heyse S, Johnston C Jr, Lindsay R (1998) Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 8:468–489
Looker AC, Melton LJ 3rd, Borrud LG, Shepherd JA (2012) Lumbar spine bone mineral density in US adults: demographic patterns and relationship with femur neck skeletal status. Osteoporos Int 23(4):1351–1360. https://doi.org/10.1007/s00198-011-1693-z
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44(3):837–845
SAS Knowledge Base/Samples & SAS Notes. Sample 25017: Nonparametric comparison of areas under correlated ROC curves. http://support.sas.com/kb/25/017.html. Accessed 12 September 2017
Hosmer DW, Lemeshow S (1980) A goodness-of-fit test for the multiple logistic regression model. Communications in Statistics: Theory and Methods A10:1043–1069
Hosmer DW, Hosmer T, Le Cessie S, Lemeshow S (1997) A comparison of goodness-of-fit tests for the logistic regression model. Stat Med 16(9):965–980
SAS Institute Inc (2011) SAS/STAT 9.3 user’s guide. SAS Institute Inc., Cary, NC
R Core Team (2017). R: a language and environment for statistical computing. R foundation for statistical computing, Vienna, Austria: URL: https://www.R-project.org/
Cosman F, de Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, Lindsay R, National Osteoporosis Foundation (2014) Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 25(10):2359–2381. https://doi.org/10.1007/s00198-014-2794-2
Watts NB, Adler RA, Bilezikian JP, Drake MT, Eastell R, Orwoll ES, Finkelstein JS (2012) Osteoporosis in men: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 97(6):1802–1822. https://doi.org/10.1210/jc.2011-3045
Ettinger B, Ensrud KE, Blackwell T, Curtis JR, Lapidus JA, Orwoll ES, Osteoporotic Fracture in Men Study Research Group (2013) Performance of FRAX in a cohort of community-dwelling, ambulatory older men: the osteoporotic fractures in men (MrOS) study. Osteoporos Int 24(4):1185–1193. https://doi.org/10.1007/s00198-012-2215-3
Nayak S, Edwards DL, Saleh AA, Greenspan SL (2015) Systematic review and meta-analysis of the performance of clinical risk assessment instruments for screening for osteoporosis or low bone density. Osteoporos Int 26(5):1543–1554. https://doi.org/10.1007/s00198-015-3025-1
Hippisley-Cox J, Coupland C (2012) Derivation and validation of updated QFracture algorithm to predict risk of osteoporotic fracture in primary care in the United Kingdom: prospective open cohort study. BMJ 344:e3427. https://doi.org/10.1136/bmj.e3427
Kanis J, Oden A, Johnell O, Johansson H, DeLaet C, Brown J, Burckhardt P, Cooper C, Christiansen C, Cummings S, Eisman J, Fujiwara S, Gluer C, Goltzman D, Hans D, Krieg M-A, LaCroix A, McCloskey E, Mellstrom D, Melton LJ 3rd, Pols H, Reeve J, Sanders K, Schott A, Silman A, Torgerson D, van Staa T, Watts N, Yoshimura N (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18:1033–1046
Browner WS (2007) Predicting fracture risk: tougher than it looks. IBMS BoneKEy 4(8):226–230
Boonen S, Reginster JY, Kaufman JM, Lippuner K, Zanchetta J, Langdahl B, Rizzoli R, Lipschitz S, Dimai HP, Witvrouw R, Eriksen E, Brixen K, Russo L, Claessens F, Papanastasiou P, Antunez O, Su G, Bucci-Rechtweg C, Hruska J, Incera E, Vanderschueren D, Orwoll E (2012) Fracture risk and zoledronic acid therapy in men with osteoporosis. N Engl J Med 367(18):1714–1723. https://doi.org/10.1056/NEJMoa1204061
Zhong ZM, Chen JT (2009) Anti-fracture efficacy of risedronic acid in men: a meta-analysis of randomized controlled trials. Clin Drug Investig 29(5):349–357. https://doi.org/10.2165/00044011-200929050-00007
Compston J, Cooper A, Cooper C, Gittoes N, Gregson C, Harvey N, Hope S, Kanis JA, McCloskey EV, Poole KES, Reid DM, Selby P, Thompson F, Thurston A, Vine N, National Osteoporosis Guideline G (2017) UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos 12(1):43. https://doi.org/10.1007/s11657-017-0324-5
Acknowledgments
We acknowledge Carrie Gartland for her assistance with manuscript preparation.
Funding
The project described was funded by grant number R01 AG046294 (Gourlay, Ritter, Overman, Fine), grant number UL1TR001111 from the National Center for Advancing Translational Sciences, and grant number K24 AR048841 (Lane) from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The work of Dr. Ensrud was supported in part with resources and use of facilities at the Minneapolis VA Medical Center. The Osteoporotic Fractures in Men Study is supported by NIH funding. The following institutes provide support: the National Institute on Aging, the National Institute of Arthritis and Musculoskeletal and Skin Diseases, the National Center for Advancing Translational Sciences, and National Institutes of Health Roadmap for Medical Research under the following grant numbers: U01 AG027810, U01 AG042124, U01 AG042139, U01 AG042140, U01 AG042143, U01 AG042145, U01 AG042168, U01 AR066160, and UL1 TR000128.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The content is solely the responsibility of the authors and does not necessarily reflect the official views of the funding agencies. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or in the decision to submit the manuscript for publication. Dr. Cawthon reports research grants from GlaxoSmithKline. Dr. Orwoll has received research and consulting support from Merck, Eli Lilly, and Amgen. Dr. Lane has received research and or consulting support from Merck, Amgen, and Regeneron. Dr. Kado has received consultant support from Kalytera Therapeutics, Takeda Pharmaceuticals, and Amgen. No other financial disclosures were reported by the authors of this paper.
Additional information
A correction to this article is available online at https://doi.org/10.1007/s11657-017-0394-4.
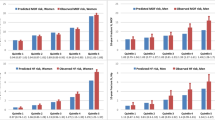
The original online version of this article was revised: The FRAX, Garvan tool, and QFracture were poorly calibrated; calibration plots revealed that the risk scores underestimated observed hip fracture incidence in the lowest deciles of scores and overestimated observed hip fracture incidence in the highest deciles of scores (Fig. 1). was corrected to The FRAX, Garvan tool, and QFracture were poorly calibrated; calibration plots revealed that the risk scores overestimated observed hip fracture incidence in the lowest deciles of scores and underestimated observed hip fracture incidence in the highest deciles of scores (Fig. 1).
Electronic supplementary material
ESM 1
(DOCX 171 kb)
Rights and permissions
About this article

Cite this article
Gourlay, M.L., Ritter, V.S., Fine, J.P. et al. Comparison of fracture risk assessment tools in older men without prior hip or spine fracture: the MrOS study. Arch Osteoporos 12, 91 (2017). https://doi.org/10.1007/s11657-017-0389-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-017-0389-1