
Abstract
Background
The Centers for Medicare and Medicaid Services’ Hospital Value-Based Purchasing program uses 30-day mortality rates for acute myocardial infarction, heart failure, and pneumonia to evaluate US hospitals, but does not account for neighborhood socioeconomic disadvantage when comparing their performance.
Objective
To determine if neighborhood socioeconomic disadvantage is associated with worse 30-day mortality rates after a hospitalization for acute myocardial infarction (AMI), heart failure (HF), or pneumonia in the USA, as well as within the subset of counties with a high proportion of Black individuals.
Design and Participants
This retrospective, population-based study included all Medicare fee-for-service beneficiaries aged 65 years or older hospitalized for acute myocardial infarction, heart failure, or pneumonia between 2012 and 2015.
Exposure
Residence in most socioeconomically disadvantaged vs. less socioeconomically disadvantaged neighborhoods as measured by the area deprivation index (ADI).
Main Measure(s)
All-cause mortality within 30 days of admission.
Key Results
The study included 3,471,592 Medicare patients. Of these patients, 333,472 resided in most disadvantaged neighborhoods and 3,138,120 in less disadvantaged neighborhoods. Patients living in the most disadvantaged neighborhoods were younger (78.4 vs. 80.0 years) and more likely to be Black adults (24.6% vs. 7.5%) and dually enrolled in Medicaid (39.4% vs. 21.8%). After adjustment for demographics (age, sex, race/ethnicity), poverty, and clinical comorbidities, 30-day mortality was higher among beneficiaries residing in most disadvantaged neighborhoods for AMI (adjusted odds ratio 1.08, 95% CI 1.06–1.11) and pneumonia (aOR 1.05, 1.03–1.07), but not for HF (aOR 1.02, 1.00–1.04). These patterns were similar within the subset of US counties with a high proportion of Black adults (AMI, aOR 1.07, 1.03–1.11; HF 1.02, 0.99–1.05; pneumonia 1.03, 1.00–1.07).
Conclusions
Neighborhood socioeconomic disadvantage is associated with higher 30-day mortality for some conditions targeted by value-based programs, even after accounting for individual-level demographics, clinical comorbidities, and poverty. These findings may have implications as policymakers weigh strategies to advance health equity under value-based programs.
Similar content being viewed by others

INTRODUCTION
As the USA shifts towards a value-based health care system, the Centers for Medicare and Medicaid Services (CMS) has implemented national programs that aim to improve quality of care and patient outcomes.1 In 2008, CMS began publicly reporting 30-day mortality rates for Medicare beneficiaries hospitalized with acute myocardial infarction (AMI), heart failure (HF), and pneumonia. Three years later, the Hospital Value-Based Purchasing Program (HVBP) was implemented, which financially penalizes or rewards hospitals based on mortality rates for these common conditions, among other measures.
Despite early enthusiasm for HVBP, there has been growing concern among policymakers and clinicians that the program may be penalizing hospitals for serving socioeconomically disadvantaged populations, rather than for poor quality care, because risk adjustment methods used by CMS do not directly account for social risk factors.2,3,4,5 A large body of work has shown that individual-level markers of poverty in the Medicare population, such as dual enrollment in Medicaid, are associated with worse outcomes.3,4,6 There is also growing awareness that neighborhood-level factors may also be associated with incident disease and care utilization, such as readmissions.3,7,8 However, less is known about the association between neighborhood socioeconomic disadvantage and mortality rates for conditions that are the targeted by the HVBP.
The Area Deprivation Index, a validated composite measure of 17 poverty, education, housing, and employment indicators, is a useful tool to granularly and comprehensively evaluate the socioeconomic context of patients’ neighborhood.8,9 Prior studies that have focused on the relationship between neighborhood disadvantage and clinical outcomes have been limited to less comprehensive definitions based solely on income,10,11 have not focused on mortality, or have been restricted to single or multi-center populations.8,12,13 In addition, few analyses have examined the intersection between the area deprivation index, the racial composition of neighborhoods, and mortality. Black Americans disproportionately experience inadequate housing conditions, poor transportation infrastructure, economic instability, and disparities in educational and employment opportunities, due to systemic inequities and structural racism.14 At the same time, Black adults are more likely to be cared for at hospitals that are disproportionately penalized by the HVBP, raising concern that the program may be perpetuating inequities in care.15
Understanding the relationship of socioeconomic disadvantage and mortality for AMI, HF, and pneumonia on a national scale, as well as in the subset of communities with a higher proportion of Black adults, is critically important, and could inform ongoing efforts to design more equitable value-based programs. Therefore, in this study, we aimed to answer the following key questions. First, among Medicare fee-for-service beneficiaries aged 65 years or older, is neighborhood socioeconomic disadvantage associated with worse 30-day mortality rates after a hospitalization for acute myocardial infarction, heart failure, or pneumonia. Second, does neighborhood socioeconomic disadvantage confer additional risk beyond individual-level demographics and poverty (e.g., dual enrollment), and if so, is this relationship explained by other factors, such as hospital characteristics or residence in rural areas? And finally, what is the association between neighborhood socioeconomic disadvantage and mortality for these conditions within Black communities in the USA?
METHODS
Institutional review board approval, including waiver of the requirement of participant informed consent, was provided by the Beth Israel Deaconess Medical Center.
Study Population
We used Medicare Provider Analysis and Review inpatient files to identify Medicare fee-for-service beneficiaries aged 65 years or older with a principal discharge diagnosis of acute myocardial infarction, heart failure, or pneumonia from January 1st, 2012, to September 30th, 2015. Study cohorts were defined using International Classification of Diseases, Ninth Revision, Clinical Modification codes used in the publicly reported CMS mortality measures. Medicare denominator files were used to identify patient demographics (age, sex, race/ethnicity), dual enrollment status, and 9-digit zip code of residence. For Medicare patients with multiple hospitalizations over the study period, we randomly selected one hospitalization per beneficiary. We excluded patients who were discharged against medical advice, were not enrolled in Medicare fee-for-service for at least 30 days after discharge (absent death), or were enrolled in Medicare for less than 1 year before hospitalization. Transfers to other hospitals were linked to their index hospitalization.
Clinical comorbidities were defined using CMS hierarchical condition categories based on Medicare inpatient claims up to 1 year before hospitalization, and diagnosis codes per claim were limited to the first 10 codes.16 Hospital characteristics were identified from the American Hospital Association file. Rurality was defined based on the 2010 Census Urban and Rural Classification as the percent of a county’s population living in a rural area.17 We also identified high-proportion Black counties using data from the US Census Bureau (2015), defined as those in the top quintile nationally in terms of the percentage of the total population that was comprised of Black individuals.
Neighborhood Socioeconomic Disadvantage
The neighborhood of residence for each Medicare beneficiary was identified using 9-digit zip codes available in the Medicare denominator file. Each beneficiary’s 9-digit zip code was then linked to an area deprivation index (ADI) score. The ADI uses an aggregate of 17 poverty, education, housing, and employment indicators drawn from US Census Data to measure neighborhood socioeconomic disadvantage (eTable 1). The 17 indicators are weighted using factor score coefficients, multiplied by their factor weights, and then summed for each geographic unit. The result is then transformed into a standardized index of percentiles where neighborhoods with higher ADI scores have higher levels of deprivation (eTable 1).8,9 Prior national analyses of Medicare beneficiaries have demonstrated a threshold effect, with a marked increase in morbidity among the top 15% most disadvantaged neighborhoods nationally by ADI.8,13 Therefore, we stratified Medicare beneficiaries according to whether they resided in the most disadvantaged neighborhoods (top 15% of ADI nationally) or in less disadvantaged neighborhoods (bottom 85% of ADI nationally)( 1).

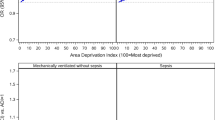
Observed 30-day mortality rates among Medicare patients hospitalized for acute myocardial infarction, heart failure, and pneumonia by neighborhood socioeconomic disadvantage. The figure shows observed all-cause 30-day post-admission mortality rates among Medicare beneficiaries aged 65 years or older hospitalized with acute myocardial infarction, heart failure, or pneumonia. Most disadvantaged neighborhoods reflect those among the top 15% most disadvantaged neighborhoods nationally, according to the area deprivation index.
Outcomes
The primary outcome was all-cause mortality within 30 days of admission among Medicare beneficiaries hospitalized for acute myocardial infarction, heart failure, or pneumonia.
Statistical Analysis
Continuous variables were summarized by mean and standard deviation; categorical variables were summarized by count and percentage. To examine the association of neighborhood socioeconomic disadvantage (most vs. less disadvantaged) with 30-day mortality for each individual condition (acute myocardial infarction, heart failure, pneumonia), we fit a generalized linear mixed-effects model with logit link function with 30-day mortality as the outcome; most disadvantaged neighborhood, age, sex, and race/ethnicity as the fixed effects; and hospital as the random effect. To understand the individual-level effect of poverty, we additionally adjusted for dual enrollment status, as well as clinical comorbidities, which represent our main findings. Next, to examine the extent which observed associations were explained by hospital-level factors that have been previously shown to influence mortality, we included key hospital characteristics including ownership, teaching status, and cardiac catheterization volume as fixed effects, in our models.18 We also adjusted for residency in a rural area, treating the rurality of each patient’s zip code as a continuous variable, as well as US region (based on the 9 US Census Bureau regions).19
To better understand the interplay between structural racism, neighborhood disadvantage, and clinical outcomes, we repeated our main analysis and evaluated the association between neighborhood socioeconomic disadvantage and mortality specifically among beneficiaries from the subset of counties with a high proportion of Black individuals.
All analyses were performed using SAS 9.3 (SAS Institute. SAS Statistical Software. 9.3 ed. Cary, NC: SAS Institute; 2011).
RESULTS
Study Population
A total of 3,471,592 Medicare patients (mean [SD] age, 79.8 [9.0]; 52.8% female) with a principal discharge diagnosis of acute myocardial infarction, heart failure, or pneumonia from January 1st, 2012, to September 30th, 2015, were included in the final study cohort. Medicare patients residing in the most disadvantaged neighborhoods, compared to those living in less disadvantaged neighborhoods, were younger (78.4 [SD 9.0] vs. 80.0 [SD 9.0] years), more likely to be Black (24.6% vs. 7.5%), dually enrolled in Medicare and Medicaid (39.6% vs. 21.8%), and reside in rural areas (34.1% vs. 23.4%) (Table 1). The burden of clinical comorbidities was generally greater among patients living in most disadvantaged areas. Patients residing in most disadvantaged neighborhoods were more likely to be admitted to public/government hospitals (13.3% vs. 9.3%), for-profit hospitals (20.3% vs.16.4%), and hospitals with low cardiac catheterization laboratory volumes (39.1% vs. 33.9%) (Table 2).
Clinical Outcomes
Medicare beneficiaries living in most disadvantaged neighborhoods, compared with those living in less disadvantaged neighborhoods, had higher observed 30-day mortality rates for acute myocardial infarction (14.3% vs. 13.4%) and pneumonia (12.8% vs. 12.2%), but not for heart failure (11.7% vs. 12.9%) (Fig. 1).
After adjustment for age, sex, and race/ethnicity, 30-day mortality rates were higher among patients from most disadvantaged neighborhoods for all three conditions (acute myocardial infarction (aOR 1.12, 95% CI 1.10–1.15), heart failure (aOR 1.03, 95% CI 1.01–1.04), and pneumonia (aOR 1.07, 95% CI 1.05–1.09)) (Table 3). These patterns persisted after also accounting for dual enrollment in Medicare and Medicaid, an individual-level marker of poverty, for acute myocardial infarction (aOR 1.09, 95% CI 1.06–1.11) and pneumonia (aOR 1.06, 95% CI 1.04–1.08), although the observed association between neighborhood disadvantage and heart failure mortality was attenuated (aOR 1.02, 95% CI 1.00–1.04). Overall findings were similar after additional adjustment for clinical comorbidities. After also including key hospital characteristics (teaching status, ownership status, cardiac catheterization volume) in our models, 30-day mortality rates remained higher among patients residing in the most disadvantaged neighborhoods for acute myocardial infarction (aOR 1.07, 95% CI 1.05–1.10) and pneumonia (aOR 1.05, 95% CI 1.03–1.07), but not for heart failure (aOR, 1.02, 95% CI 1.00–1.04). These findings were similar after additionally adjusting for rurality of residence and US region.
As an additional analysis, we focused on the subset of counties with high proportion of Black adults (eTable 2). Similar to our main findings, within high-proportion Black counties, beneficiaries from the most disadvantaged neighborhoods (relative to those in less disadvantaged areas) were at higher risk of 30-day mortality for acute myocardial infarction (aOR 1.07, 95% CI 1.03–1.11) and pneumonia (aOR 1.03, 95% CI 1.00-1.07), but not for heart failure (aOR 1.02, 95% CI 0.99–1.05), after adjustment for demographics, dual enrollment, and clinical comorbidities (Table 4).
DISCUSSION
In this study, we found that Medicare beneficiaries ≥65 years of age residing in the most socioeconomically disadvantaged neighborhoods had higher 30-day mortality rates after a hospitalization for acute myocardial infarction and pneumonia compared with those living in less disadvantaged neighborhoods. The association between neighborhood socioeconomic disadvantage and increased risk of mortality persisted even after accounting for demographics, clinical comorbidities, and importantly, individual-level markers of poverty. These patterns were similar even when we restricted our analysis to US counties with a high proportion of Black residents. Our findings are consistent with a prior study of the Medicare population, which explored the relationship between neighborhood socioeconomic disadvantage (based on the area deprivation index) and readmissions for AMI, HF, and pneumonia.8 We extend upon this evidence by demonstrating that on a national scale, neighborhood disadvantage is independently associated with higher 30-day mortality rates in the Medicare population, even after accounting for individual-level poverty, for some conditions targeted by the HVBP.
In the USA, there has been increasing concern that value-based programs may disproportionately penalize clinicians and health systems for serving poor and vulnerable patients rather than for lower quality care. Safety-net hospitals and outpatient practices that care for low-income populations, for example, fare worse under value-based programs.5,20,21,22 In addition, recent evidence suggests that hospitals that care for a high proportion of Black adults are disproportionately penalized by value-based programs like the HVBP, even after accounting for safety-net status.15 Hospitals that predominately care for low-income and racial/ethnic minority communities tend to be under-resourced and have lower operating margins. The HVBP rewards or penalizes hospitals up to 2% of Medicare payments, and small shifts in payment adjustments under the HVBP may have big implications for the financial sustainability of safety-net sites, and more broadly, the health and economic welfare (e.g., unemployment due to hospital closures) of the communities they serve. As value-based programs and alternative payment models (APM) proliferate, policymakers should ensure that these policies prioritize health equity,2,23 and consider accounting for both individual- and neighborhood-level markers of socioeconomic disadvantage to fairly compare health care system performance.
Our findings also demonstrate that a disproportionate number of Black beneficiaries live in the most disadvantaged neighborhoods in the USA. Nearly 1 in 4 Medicare beneficiaries living in the most disadvantaged neighborhoods across the country were Black adults — more than 3-fold greater than the proportion in less disadvantaged neighborhoods. These differences reflect ongoing residential and economic segregation in the USA,24,25 which has been driven by structural racism, and has led to Black communities experiencing worse access to care, including provider shortages and pharmacy deserts, as well as greater exposure to unique sources of chronic stress.14,18,19,26 Even after we restricted our analysis to the subset of US counties with a high proportion of Black adults, patients from most disadvantaged neighborhoods experienced higher death rates after a hospitalization for acute myocardial infarction or pneumonia, compared to those from less disadvantaged neighborhoods in these counties.
The association between neighborhood socioeconomic disadvantage and individual health is complex, and there are several potential explanations for why in the current study, patients from disadvantaged neighborhoods experienced worse outcomes after a hospitalization for acute myocardial infarction or pneumonia. The characteristics of a community may shape and reinforce the persistence of established risk factors for specific conditions, such as cardiovascular disease,27 and neighborhoods differ in the availability and cost of healthy foods, accessibility, and quality of public spaces and recreational facilities, as well as adequacy of medical supplies.18,19,28,29 In addition, it is possible that lower quality hospitals are more likely to be located in disadvantaged communities. Finally, living in a socioeconomically disadvantaged neighborhood is associated with worse access to post-discharge care, including close outpatient follow-up and cardiac rehabilitation,30 both of which are associated with better outcomes.31,32 Collectively, these factors may contribute to higher death rates in socioeconomically disadvantaged neighborhoods, and more broadly, suggest that strategies to improve health outcomes may need to combine person-centered approaches with initiatives aimed at improving residential communities.
In contrast to acute conditions targeted by the HVBP (myocardial infarction, pneumonia), patients from most disadvantaged neighborhoods who were hospitalized with heart failure did not experience worse mortality rates. It is possible that the factors associated with neighborhood disadvantage (e.g., poor outpatient follow-up, pharmacy deserts, worse access to cardiac rehabilitation, or high-quality skilled nursing facilities) have a more salient impact on outcomes during the vulnerable 30-day period after a hospitalization for acute, potentially life-threatening, conditions (e.g., myocardial infarction), while these factors exert their effect on patients with chronic conditions — like heart failure — over a longer time horizon. Other potential explanations pertain to our observation that Medicare patients residing in disadvantaged areas were 3 times more likely to be Black beneficiaries. Although younger (<65 years) Black adults have markedly higher heart failure–related mortality rates compared with White adults in the USA,33 older Black adults in the Medicare population experience lower mortality rates after a heart failure hospitalization.10,34,35 These patterns may partially reflect survivorship bias given the higher premature mortality rates in the Black population. In addition, Black adults with heart failure have a higher prevalence of salt sensitivity and may be more prone to sudden symptomatic pulmonary congestion.36,37 As a result, severity of illness in this population may be lower at the time of hospitalization in ways that were not captured in our study. Finally, and perhaps most importantly, resiliency may contribute to lower mortality among older Black adults with chronic conditions — like heart failure — in the face of greater exposure to negative risk factors, including a disproportionate burden of social, economic, and environmental barriers and adversities.38 Future research is needed to understand how risks and strengths in the social environment are structurally patterned by race, ethnicity, and socioeconomic status at both the individual and neighborhood levels, and the impact of these structural inequities on cardiovascular disease and other health outcomes.39,40
Limitations
This study has several limitations. First, this study focused on Medicare fee-for-service beneficiaries aged 65 years or older, as hospitalization-related information about the managed care (Medicare Advantage) population is not available for the years of our study. Examining clinical outcomes in the managed care population by neighborhood socioeconomic disadvantage will be an important area for further research. Second, we used administrative data linked to the area deprivation index (ADI), but lacked granular detail on other important factors such as social support and health literacy. Nonetheless, the ADI incorporates 17 indicators of poverty, education, housing, and employment, and therefore provides a more comprehensive measure of neighborhood socioeconomic disadvantage than neighborhood income alone. Third, we were unable to disentangle the extent to which worse outcomes among beneficiaries from the most disadvantaged areas were driven by the delivery of lower quality care, and it is possible that hospital quality mediates the relationship between neighborhood disadvantage and mortality — this remains an important area for future study. Fourth, although the magnitude of the association between the area deprivation index and mortality that we observed was similar to prior evaluations of the Medicare population that have focused on 30-day readmissions,8 we did not assess the extent to which would change payment adjustments under the HVBP, which should be explored future work. Fifth, neighborhood socioeconomic disadvantage was based on the zip code of residence for each beneficiary from 2012 to 2015, and we were unable to account for cumulative exposure to disadvantaged neighborhoods prior to the study period.41
CONCLUSION
Medicare beneficiaries residing in the most socioeconomically disadvantaged neighborhoods had higher 30-day mortality rates after a hospitalization for acute myocardial infarction and pneumonia compared with those living in less disadvantaged neighborhoods, even after accounting for individual-level demographics, clinical comorbidities, and poverty. The association between neighborhood disadvantage and mortality was similar within the subset of US counties with a high proportion of Black residents. These findings may have important implications as CMS weighs strategies to advance health equity under value-based programs, and indicate that policymakers should consider accounting for neighborhood-level markers of socioeconomic disadvantage to ensure fair comparisons of health system performance.
References
Woolf SH, Schoomaker H. Life expectancy and mortality rates in the United States, 1959-2017. JAMA. 2019;322(20):1996-2016.
Joynt Maddox KE. Financial incentives and vulnerable populations - will alternative payment models help or hurt? N Engl J Med. 2018;378(11):977-979.
Joynt Maddox KE, Reidhead M, Hu J, et al. Adjusting for social risk factors impacts performance and penalties in the hospital readmissions reduction program. Health Serv Res. 2019;54(2):327-336.
Roberts ET, Zaslavsky AM, Barnett ML, Landon BE, Ding L, McWilliams JM. Assessment of the effect of adjustment for patient characteristics on hospital readmission rates: implications for pay for performance. JAMA Intern Med. 2018;178(11):1498-1507.
Ryan AM. Will value-based purchasing increase disparities in care? N Engl J Med. 2013;369(26):2472-2474.
Wadhera RK, Wang Y, Figueroa JF, Dominici F, Yeh RW, Joynt Maddox KE. Mortality and hospitalizations for dually enrolled and nondually enrolled Medicare beneficiaries aged 65 years or older, 2004 to 2017. JAMA. 2020;323(10):961-969.
Report to Congress: Social risk factors and performance under Medicare’s value-based purchasing programs. U.S. Department of Health & Human Services, Office of the Assistant Secretary for Planning and Evaluation Web site. https://aspe.hhs.gov/pdf-report/report-congress-social-risk-factors-and-performance-under-medicares-value-based-purchasing-programs Published 2016. Accessed 2019, April.
Kind AJ, Jencks S, Brock J, et al. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study. Ann Intern Med. 2014;161(11):765-774.
Kind AJH, Buckingham WR. Making neighborhood-disadvantage metrics accessible - The neighborhood atlas. N Engl J Med. 2018;378(26):2456-2458.
Downing NS, Wang C, Gupta A, et al. Association of racial and socioeconomic disparities with outcomes among patients hospitalized with acute myocardial infarction, heart failure, and pneumonia: an analysis of within- and between-hospital variation. JAMA Netw Open. 2018;1(5):e182044.
Bernheim SM, Parzynski CS, Horwitz L, et al. Accounting for patients' socioeconomic status does not change hospital readmission rates. Health Aff (Millwood). 2016;35(8):1461-1470.
Berman AN, Biery DW, Ginder C, et al. Association of socioeconomic disadvantage with long-term mortality after myocardial infarction: the Mass General Brigham YOUNG-MI Registry. JAMA Cardiol. 2021.
Hu J, Kind AJH, Nerenz D. Area deprivation index predicts readmission risk at an urban teaching hospital. Am J Med Qual. 2018;33(5):493-501.
Bailey ZD, Krieger N, Agenor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389(10077):1453-1463.
Aggarwal R, Hammond JG, Joynt Maddox KE, Yeh RW, Wadhera RK. Association between the proportion of black patients cared for at hospitals and financial penalties under value-based payment programs. JAMA. 2021;325(12):1219-1221.
Tsugawa Y, Figueroa JF, Papanicolas I, Orav EJ, Jha AK. Assessment of strategies for managing expansion of diagnosis coding using risk-adjustment methods for Medicare data. JAMA Intern Med. 2019.
2010 Census Urban and Rural Classification and Urban Area Criteria. United States Census Bureau. United States Census Bureau Web site. https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html. Published 2019. Accessed January 2, 2020.
Amstislavski P, Matthews A, Sheffield S, Maroko AR, Weedon J. Medication deserts: survey of neighborhood disparities in availability of prescription medications. Int J Health Geogr. 2012;11:48.
Bower KM, Thorpe RJ, Rohde C, Gaskin DJ. The intersection of neighborhood racial segregation, poverty, and urbanicity and its impact on food store availability in the United States. Prev Med. 2014;58:33-39.
Joynt KE, Jha AK. Characteristics of hospitals receiving penalties under the Hospital Readmissions Reduction Program. JAMA. 2013;309(4):342-343.
Sankaran R, Sukul D, Nuliyalu U, et al. Changes in hospital safety following penalties in the US Hospital Acquired Condition Reduction Program: retrospective cohort study. BMJ. 2019;366:l4109.
Wadhera RK, Bhatt DL, Kind AJH, et al. Association of outpatient practice-level socioeconomic disadvantage with quality of care and outcomes among older adults with coronary artery disease: implications for value-based payment. Circ Cardiovasc Qual Outcomes. 2020:CIRCOUTCOMES119005977.
Wadhera RK, Yeh RW, Joynt Maddox KE. The Hospital Readmissions Reduction Program - time for a reboot. N Engl J Med. 2019;380(24):2289-2291.
Massey D. Residential segregation and neighborhood conditions in U.S. Metropolitan areas. In: Smelser NJ WW, Mitchell F, ed. America Becoming: Racial Trends and Their Consequences, Volume 1. Washington, DC: The National Academies Press; 2001:391-434.
Firebaugh G, Acciai F. For blacks in America, the gap in neighborhood poverty has declined faster than segregation. Proc Natl Acad Sci U S A. 2016;113(47):13372-13377.
Gaskin DJ, Dinwiddie GY, Chan KS, McCleary RR. Residential segregation and the availability of primary care physicians. Health Serv Res. 2012;47(6):2353-2376.
Diez Roux AV, Merkin SS, Arnett D, et al. Neighborhood of residence and incidence of coronary heart disease. N Engl J Med. 2001;345(2):99-106.
Lee JG, Henriksen L, Rose SW, Moreland-Russell S, Ribisl KM. A systematic review of neighborhood disparities in point-of-sale tobacco marketing. Am J Public Health. 2015;105(9):e8-18.
Hirsch JA, Moore KA, Clarke PJ, et al. Changes in the built environment and changes in the amount of walking over time: longitudinal results from the multi-ethnic study of atherosclerosis. Am J Epidemiol. 2014;180(8):799-809.
Castellanos LR, Viramontes O, Bains NK, Zepeda IA. Disparities in cardiac rehabilitation among individuals from racial and ethnic groups and rural communities-a systematic review. J Racial Ethn Health Disparities. 2019;6(1):1-11.
Anderson L, Oldridge N, Thompson DR, et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67(1):1-12.
Ayanian JZ, Landrum MB, Guadagnoli E, Gaccione P. Specialty of ambulatory care physicians and mortality among elderly patients after myocardial infarction. N Engl J Med. 2002;347(21):1678-1686.
Glynn P, Lloyd-Jones DM, Feinstein MJ, Carnethon M, Khan SS. Disparities in cardiovascular mortality related to heart failure in the United States. J Am Coll Cardiol. 2019;73(18):2354-2355.
Huckfeldt P, Escarce J, Sood N, Yang Z, Popescu I, Nuckols T. Thirty-day postdischarge mortality among Black and White patients 65 years and older in the Medicare Hospital Readmissions Reduction Program. JAMA Netw Open. 2019;2(3):e190634.
Wadhera RK, Joynt Maddox KE, Wasfy JH, Haneuse S, Shen C, Yeh RW. Association of the Hospital Readmissions Reduction Program with mortality among Medicare beneficiaries hospitalized for heart failure, Acute Myocardial Infarction, and Pneumonia. JAMA. 2018;320(24):2542-2552.
Nayak A, Hicks AJ, Morris AA. Understanding the complexity of heart failure risk and treatment in Black patients. Circ Heart Fail. 2020;13(8):e007264.
Deswal A, Petersen NJ, Souchek J, Ashton CM, Wray NP. Impact of race on health care utilization and outcomes in veterans with congestive heart failure. J Am Coll Cardiol. 2004;43(5):778-784.
Kim JH, Islam SJ, Topel ML, et al. Individual psychosocial resilience, neighborhood context, and cardiovascular health in Black adults: a multilevel investigation from the Morehouse-Emory Cardiovascular Center for Health Equity Study. Circ Cardiovasc Qual Outcomes. 2020;13(10):e006638.
Pager D, Shepherd H. The sociology of discrimination: racial discrimination in employment, housing, credit, and consumer markets. Annu Rev Sociol. 2008;34:181-209.
Braveman PA, Cubbin C, Egerter S, Williams DR, Pamuk E. Socioeconomic disparities in health in the United States: what the patterns tell us. Am J Public Health. 2010;100 Suppl 1(Suppl 1):S186-196.
Jones NL, Gilman SE, Cheng TL, Drury SS, Hill CV, Geronimus AT. Life course approaches to the causes of health disparities. Am J Public Health. 2019;109(S1):S48-S55.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Wadhera receives research support from the National Heart, Lung, and Blood Institute (grant K23HL148525-1) at the National Institutes of Health. He serves as consultant for Abbott, outside the submitted work. Dr. Joynt Maddox receives research support from the National Heart, Lung, and Blood Institute (R01HL143421) and National Institute on Aging (R01AG060935). Dr. Shen is currently employed by Biogen, but contributed to this work when he was the Statistical Director at the Richard A. and Susan F. Smith Center for Outcomes Research at Beth Israel Deaconess Medical Center. Dr. Yeh receives research support from the National Heart, Lung and Blood Institute (R01HL136708) and the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology and receives personal fees from Biosense Webster, grants and personal fees from Abbott Vascular, AstraZeneca, Boston Scientific, and Medtronic, outside the submitted work. All other authors have no disclosures.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 5743 kb)
Rights and permissions
About this article

Cite this article
Hermes, Z., Joynt Maddox, K.E., Yeh, R.W. et al. Neighborhood Socioeconomic Disadvantage and Mortality Among Medicare Beneficiaries Hospitalized for Acute Myocardial Infarction, Heart Failure, and Pneumonia. J GEN INTERN MED 37, 1894–1901 (2022). https://doi.org/10.1007/s11606-021-07090-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-021-07090-z