
Abstract
Background
In 2015, the US Preventive Services Task Force (USPSTF) revised clinical recommendations to more broadly recommend abnormal blood glucose screening and more clearly recommend referral to behavioral interventions for adults with prediabetes.
Objective
To assess the effects of the 2015 USPSTF recommendation changes on abnormal blood glucose screening and referral to behavioral interventions, and to examine physicians’ perceptions of the revised recommendation.
Design
We utilized a sequential, dependent mixed-methods triangulation design.
Participants
A total of 33,444 patients meeting USPSTF abnormal blood glucose screening criteria within 15 health system–affiliated primary care practices and 20 primary care physicians in North Carolina.
Main Measures
We assessed monthly abnormal blood glucose screening rate and monthly referral rate to behavioral interventions. To estimate trend changes in outcomes, we used segmented linear regression analysis of interrupted time-series data. We gathered physicians’ perspectives on the 2015 USPSTF abnormal blood glucose recommendation including awareness of, agreement with, adoption of, and adherence to the recommendation. To analyze qualitative data, we used directed content analysis.
Key Results
There was a slight significant change in trend in abnormal blood glucose screening rates post-recommendation. There was a slight, statistically significant decrease in referral rates to behavioral interventions post-recommendation. Physicians were generally unaware of the revisions to the 2015 USPSTF abnormal blood glucose recommendation; however, once the recommendations were described, physicians agreed with the screening recommendation but felt that the behavioral intervention referral recommendation was hard to implement.
Conclusion
The 2015 USPSTF abnormal blood glucose guideline had little to no effect on abnormal blood glucose screening or referral to behavioral interventions in North Carolina practices. Potential interventions to improve these rates could include clinical decision tools embedded in the electronic health record and better referral systems for community-based diabetes prevention programs.
Similar content being viewed by others

INTRODUCTION
In 2015, 84.1 million American adults had prediabetes, a condition in which blood glucose levels are elevated but not high enough to be classified as diabetes.1 Unfortunately, many adults with prediabetes are unaware of their prediabetes status and prediabetes often goes untreated in primary care resulting in missed opportunities to prevent or delay progression to diabetes.2,3,4,5
In October 2015, the US Preventive Services Task Force (USPSTF) updated its abnormal blood glucose clinical recommendations to advise clinicians to screen all adults who are overweight or obese and aged 40 to 70 years for abnormal blood glucose and refer those with prediabetes-range levels to intensive behavioral interventions.6 The previous guideline only recommended routine abnormal blood glucose screening in adults with hypertension with no clear recommendation for follow-up care. This updated recommendation reports moderate to strong data indicating that a substantial proportion of diabetes cases can be delayed or prevented if addressed in the prediabetes stage.6
Unfortunately, only one-third of evidence-based clinical guidelines are routinely adhered to in practice.7 Based on the Awareness-to-Adherence Model of Clinical Guideline Compliance, clinicians’ adherence to clinical guidelines occurs through four sequential steps.8 Physicians must first become aware of the specific guideline, then must intellectually agree with it, then decide to adopt it, then succeed in adhering to it.8 Little is known about the extent to which clinicians are aware of, agree with, and have adopted the 2015 USPSTF abnormal blood glucose recommendations.
The objectives of this mixed-methods study were to (1) assess the effects of the 2015 USPSTF recommendation changes on diabetes screening rates and rates of referral to behavioral interventions for adults with prediabetes; and (2) examine physicians’ perceptions of the 2015 USPSTF clinical guideline.
METHODS
Study Design
This study implemented a sequential-dependent mixed-methods triangulation design to combine two studies, a quantitative retrospective cohort study and qualitative in-depth interviews.9 Data integration occurred in interpretation to corroborate each study’s findings.10, 11 The quantitative analytic research was conducted in health system–affiliated primary care practices in rural, urban, and suburban locations across North Carolina and involved secondary analysis of existing longitudinal electronic health record (EHR) data. The qualitative study was conducted with physicians in two medical school–affiliated family medicine and internal medicine practices within this study’s health system. As part of the mixed-methods approach, we used the quantitative dataset to generate the physician sampling frame for the qualitative interviews with primary care physicians (PCPs). All study procedures and materials were reviewed and approved by the institutional review board at the University of North Carolina at Chapel Hill (#17-2610).
Overview of Study Data
Quantitative Data
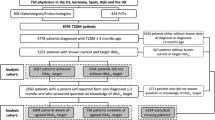
We aggregated EHR data from patients from fifteen primary care practices affiliated with an academic health system who met the following inclusion criteria during the entire study period from 5/1/2014 to 4/30/2017: (1) at least one visit to an affiliated primary care practice; and (2) met the 2015 USPSTF screening criteria (i.e., body mass index ≥ 25 kg/m2 and age of 40 to 70 years). To restrict to those at risk of incident diabetes and those eligible for screening according to the 2015 USPSTF recommendation, we excluded patients diagnosed with diabetes, hyperglycemia, abnormal glucose, impaired glucose tolerance, impaired fasting glucose, or prediabetes before the study period. We also excluded pregnant women, as gestational diabetes screening and treatment are covered by a different USPSTF recommendation.
Interrupted Time-Series Analysis
Outcomes and Measures
The two primary outcomes were monthly abnormal blood glucose screening rate and monthly referral rate to behavioral interventions. The monthly abnormal blood glucose screening rate was defined as the number of patients who had documented receipt of a hemoglobin A1c (HbA1c) test, a fasting blood glucose (FBG) test, or an oral glucose tolerance test (OGTT) each month divided by the number of patients with a health system–affiliated primary care visit who were eligible for screening (i.e., met the 2015 USPSTF screening criteria) that month. The monthly rate of referral to behavioral interventions was defined as the number of patients with a prediabetes-range laboratory value who had an EHR-documented, ambulatory referral to a nutritionist, diabetes education, or weight management program within 6 months of their screening test, divided by the total person-days in that month. Person-days were used to reflect a more accurate referral rate estimate rather than a simple monthly count, which would tend to underestimate the occurrence of referrals. The number of person-days a patient contributed to the study was calculated as referral date minus screening date (for those referred within 6 months of screening), or as screening date plus 180 days (for those not referred).
Statistical Analyses
To estimate trend changes in diabetes screening rates and rates of referral to behavioral interventions, we used segmented linear regression analysis of interrupted time-series data,12, 13 a quasi-experimental method to assess trend changes occurring after clearly defined events in time.
We identified two time-based interruptions when we hypothesized that the USPSTF recommendation changes could have altered both abnormal blood glucose screening rates and rates of referral to behavioral interventions (compared to before the USPSTF recommendation changes). The two identified interruptions were (1) the online release of the 2015 recommendation on both the USPSTF website and the Annals of Internal Medicine website in October 2015; and (2) the in-print publication and dissemination of the recommendation in Annals of Internal Medicine in December 2015.6 We negatively lagged all interruptions to match each recommendation release, online and in-print, with the patients who were subject to its potential impact (i.e., those meeting the guideline’s criteria for screening).14 To control for confounding by seasonality in our analyses, we used a transformed cosine periodic function.15, 16 Between any two interruptions, the trend estimate (i.e., the change in rates during that specific time interval) was calculated from the baseline trend and the effect of each recommendation release date on the underlying trend.
We used a segmented linear regression model that included four time-based covariates for (1) pre-recommendation slope, (2) change in level at online recommendation release, (3) change in level at print recommendation release, and (4) change in slope from pre-recommendation to post-recommendation. These slopes quantified the trends for screening and referral before recommendation release, as well as the level of change that could be attributed to the online and print recommendation releases, and the level of change accounted for by the pre-recommendation trend. The change in slope quantified the difference between the pre-recommendation and post-recommendation slopes. Data management and statistical analyses were conducted by using SAS version 9.4 (SAS Institute Inc., Cary, NC). We estimated rates with corresponding 95% confidence intervals (CIs) and all trend estimates with 95% CIs.
In-depth Interviews
Qualitative data collection was conducted at the two academic-affiliated family medicine and internal medicine clinics that contributed the highest percentage of patients to the quantitative dataset, 26.4% and 17.7% respectively, within the study’s health system from October 2018 to April 2019. To determine the sampling frame for the qualitative study, we queried the quantitative dataset to identify the names of all physicians listed as a patient participant’s PCP during the study period. The resulting sampling frame was all PCPs who were both currently employed by either of the two clinics and listed as a PCP within the study’s patient sample. All 39 eligible providers were invited to participate. PCPs were recruited via email and received a $20 gift card for participation in the 30-min interview. The interviewer’s guide was informed by the Awareness-to-Adherence Model of Clinical Guideline Compliance8 and questions assessed EHR use for diabetes prevention and awareness of, agreement with, and adherence to the 2015 USPSTF abnormal blood glucose recommendation. In-depth interviews were audio-recorded and transcribed. The interviewer collected demographic information on PCP’s gender, number of years in practice, and percent of time spent seeing patients. Data was managed using Atlas.ti® 8 software.
Analysis
Methods from directed content analysis were used to analyze qualitative data.17 A codebook was developed a priori based on the Awareness-to-Adherence Model and the interview guide. This codebook was iteratively refined by reviewing the first nine transcripts and additional codes were derived by highlighting words from the text that appeared to capture key thoughts or concepts. The resulting codebook included codes from the theoretical framework, interview guide, and de novo topics identified inductively. Categories were then used to organize and group codes into meaningful clusters.17 Codes were applied to the entire dataset. Two investigators coded all interviews using the final codebook. All discrepancies between coders were reviewed and resolved through dialog between the coder and the first author. Matrices were used to visually represent data and to facilitate analysis by organizing and reducing data.
RESULTS
Interrupted Time-Series
We identified 33,444 patients with at least one primary care visit during our study period and who met the 2015 USPSTF Abnormal Blood Glucose Guideline (i.e., aged 40–70 years and BMI ≥ 25 kg/m2). We identified 5598 patients with prediabetes-ranged laboratory values (FBG: 100–125 mg/dL, HbA1C 5.7–6.4%, OGTT: 2-h glucose 140–199 mg/dL). Patient characteristics for both samples are found in Table 1. For each analysis, patient data were aggregated monthly.
Screening
Across the study period, only 20.88% of patients eligible for screening were screened for diabetes. Table 2 and Figure 1 provide the results of the segmented regression analysis assessing monthly abnormal blood glucose screening rate as the outcome. Table 2 provides the coefficients and 95% CI with statistical significance for the rate and slope before recommendation change, after online release of the recommendation, and after print release of the recommendation. The baseline screening rate was 14.63%. Overall, the slope of abnormal blood glucose screening increased by 1.14% per year before the release of the 2015 USPSTF recommendation (95% CI, 0.95 to 1.34%). There was no immediate change in screening rates after the first online release; however, after the print release (and coincidental lag of the online release), the trend for screening rates was significantly steeper compared to the pre-recommendation trend (1.41% per year in post-period [95% CI, 1.20, 1.63], p value for difference < 0.05).

Monthly percent of patients screened for abnormal blood glucose over time.
Referral to Behavioral Interventions
Across the study period, only 2.5% of patients with prediabetes were referred to behavioral interventions. Table 3 and Figure 2 provide the results of the segmented regression analysis using monthly referral to behavioral intervention as the outcome. Table 3 provides the coefficients and 95% CI for the rate and slope before recommendation change, after online release of the recommendation, and after print release of the recommendation with statistical significance. Overall, the slope increased by 3.98% per year prior to the release of the 2015 guideline (95% CI, 2.74 to 5.23%). After the online release of the guideline change, however, there was a statistically significant decrease in referral rate by 7.43% (to − 3.44% per year [95% CI, − 4.35 to − 2.53]). After the print release, the referral rate bounced upward by 3.28%, to a final slope equivalent to the horizontal, of − 0.16% (95% CI, − 0.38 to 0.05).

Monthly percent of patients referred to behavioral interventions over time.
In-depth Interviews
A total of 20 PCPs participated in interviews (52% response rate), 9 from family medicine and 11 from internal medicine. Physicians were evenly split between women and men, 80% were less than full-time in clinic and 25% had less than 10 years in practice. We organized qualitative findings using the Awareness-to-Adherence Model and present illustrative quotes related to the model in Table 4.
Awareness
Most PCPs were not only unaware of the revised 2015 USPSTF guideline but could not cite any USPSTF guideline related to abnormal blood glucose. Of those who could cite a USPSTF abnormal blood glucose recommendation, half cited the 2015 USPSTF guideline while the rest cited the 2008 guideline. Furthermore, most physicians who could recite the guideline only mentioned the screening portion of the recommendation and rarely mentioned the referral to behavioral intervention portion.
Agreement
While all PCPs agreed with the revised USPSTF screening guideline after being told about it, many physicians felt that patients with obesity younger than 40 years should also be screened and mentioned this as part of their clinical practice.
Not all PCPs agreed with the 2015 USPSTF guideline’s recommendation to refer adults found to have prediabetes to intensive behavioral interventions. Most PCPs felt that, in theory, intensive behavioral interventions were a good treatment option for prediabetes but felt that, in practice, many patients, communities, and clinics did not have the resources or time to implement and/or adhere to intensive programs.
Adoption, Adherence, and Utilization of the EHR for Diabetes Prevention
Physicians felt that they were adhering to the screening portion of the revised recommendation, even if they were not formally familiar with it. When commenting on their own screening behaviors, PCPs often stated that they were likely not screening patients who were overweight and were more likely to screen patients with obesity. Few PCPs mentioned both age and BMI, the two criteria from the 2015 USPSTF recommendation, when asked what factors they consider when deciding to screen a patient for abnormal blood glucose with most providers citing that they screened patients who were hypertensive, who “looked obese,” or who had a family history of diabetes.
Regarding referral to intensive behavioral interventions, many physicians felt conflicted. While most agreed that referral to intensive behavioral interventions was a good option for prediabetes treatment, PCPs believed that many of their patients did not have the resources (e.g., time, finances, transportation) to engage in intensive programs and that older, retired patients tended to have the time and resources to effectively engage in these programs. Many PCPs were hesitant to make inefficient referrals that their patients would not be able to undertake especially if these referrals could lead to out-of-pocket costs for their patients. Physicians were generally unaware of any available intensive programs and even if they were, they often were not aware of specific programs in patients’ communities to which they could refer. Furthermore, the health system did not have a formal process for referral to community programs and many providers were unsure how to make external referrals. Less than half of physicians stated that they referred to community programs for diabetes prevention with less than a third saying that they referred patients to the National Diabetes Prevention Program. In sum, there was little awareness of the 2015 USPSTF recommendation but much agreement with the recommendation, while recommendation adoption and adherence were low.
Overall, physicians used the EHR for diabetes prevention in the following ways: (1) to order screening tests for patients, (2) to review and communicate screening results to patients, (3) to refer patients to clinic-based nutritionists, (4) to add prediabetes to patients’ problem lists, and to (5) document behavioral counseling related to prediabetes in clinical notes.
EHR-related facilitators to diabetes prevention included the ease of ordering screening tests (for non-Medicare patients), communicating screening test results to patients (who opted in and utilized these services), and making health system–based and clinic-based referrals (for those services offered within the clinic/health system). When asked what strategies could be used to improve health system–wide diabetes prevention efforts, 70% of PCPs interviewed recommended best practice alerts as a strategy to help identify patients who needed to be screened (based on guideline recommendations) and to identify patients with prediabetes who needed behavioral referrals or counseling. The main EHR-related barrier to diabetes prevention was difficulty in referring patients to programs/services outside of the health system. For example, many physicians did not refer patients to community-based programs because there was no clear, EHR-based mechanism to do so.
DISCUSSION
Our study had several key findings that shed light on the impact that the 2015 USPSTF abnormal blood glucose recommendation had on clinical practice. First, we observed an upward trend in abnormal blood glucose screening over time, which became more pronounced after both phases of the 2015 USPSTF abnormal blood glucose recommendation release. However, in contrast to what we expected, the trend of referral rates to behavioral interventions for those identified with prediabetes, which had been increasing significantly before the USPSTF recommendations, was flattened after their release. In-depth interviews with PCPs did not elucidate reasons for this change. Of note, trend changes aside, the rates of diabetes screening and referral to behavioral interventions were low throughout the study period.
Qualitative findings utilizing Pathman’s Awareness-to-Adherence Model shed an interesting light on our quantitative findings. While our quantitative findings demonstrated low rates of screening for abnormal blood glucose and referral to behavioral interventions, most clinicians self-reported that, although they were unaware of the 2015 recommendations, once described, they believed their screening and referral behaviors aligned with them. This finding suggests that providers may substantially overestimate the extent to which they are carrying out the indicated clinical practices. In a systematic review of studies assessing the Awareness-to-Adherence Model and its application to clinical guideline implementation, Mickan et al. found that, although guideline awareness usually precedes agreement, in instances where guidelines are poorly disseminated or there is widespread consensus regarding appropriate practice, agreement can occur without awareness, as was seen in our study.7 Also consistent with our findings, Mickan et al. noted that clinicians’ self-reporting of guideline-related behaviors tends to overestimate adherence to the guideline.7
Findings from our study complement those reported by Mainous et al. and Tseng et al. which assessed physician perspectives on and knowledge of diabetes prevention strategies.18, 19 Utilizing a survey sample of 1248 family physicians, Mainous et al. found that, in regard to utilization of diabetes prevention guidelines, only 52.4% of physician participants reported following national guidelines (e.g., UPSTF or American Diabetes Association) and one-third of the respondents were uncertain whether the screening and care they provided were consistent with clinical guidelines.18 Mainous et al. also found that academic family physicians in the USA do not universally embrace screening for and treating prediabetes as a diabetes prevention strategy.18 In a survey sample of 140 primary care providers from multispecialty practices affiliated with one academic health system, Tseng et al. found that, on average, PCPs selected 8 of the 11 correct factors for abnormal blood glucose screening with only 39% of PCPs selecting all the medical risk factors recommended by published guidelines.19 Tseng et al. also found that only 11% of providers selected referral to a behavioral weight loss program as the best/recommended initial management approach for patients with prediabetes. Most providers selected lack of weight or nutrition resources, lack of motivation, and patients’ physical limitations for physical activity as barriers to lifestyle changes.19 Taken together, our studies highlight PCPs’ lack of adoption of diabetes prevention–related clinical guidelines in practice, lack of knowledge about diabetes risk factors recommended for screening, and incomplete knowledge on evidence-based recommendations for prediabetes treatment.
There are important clinical implications of our findings. In our study, many physicians were unaware of the updated screening criteria, were unaware of local options for intensive behavioral interventions to which they could refer patients, and cited the lack of a formal, health system–wide referral process as a barrier to recommendation adoption and implementation. Furthermore, most PCPs interviewed recommended best practice alerts integrated in the EHR to improve health system–wide diabetes prevention efforts. Given these findings, the EHR may be a good platform for coordinating system-wide provider- or patient-level interventions. For example, Nhim et al. found in a cross-sectional web-based survey of 2006 PCPs that the odds of screening patients for abnormal blood glucose were significantly higher among those who used EHRs to manage patients with prediabetes compared to those who did not; the odds of referring patients with prediabetes to a CDC-recognized DPP was significantly higher for providers who had heard of such programs and among providers who practiced in areas with a high ratio of programs to total PCPs.20 Moreover, Chambers et al. found that modifying the EHR system to facilitate patient referrals to the NDPP in combination with a provider education intervention increased and sustained clinic-based NDPP referrals.21 This research highlights the importance of the EHR in facilitating screening and referrals and the opportunity to automate referrals to community-based, intensive lifestyle interventions to overcome physician barriers.
Our study goes beyond prior research by simultaneously providing quantitative estimates of the implementation of the 2015 USPSTF abnormal blood glucose guideline along with qualitative insights about the factors that contributed to low implementation, including providers’ awareness, agreement, adoption, and adherence to this guideline. However, there are limitations to our study. First, our study was conducted in a single, albeit large, academic health system, which limits the internal validity of our findings—since we only had data on patients’ interactions with this healthcare system—as well as the generalizability of our findings to other contexts. Furthermore, diabetes screening and referral to behavioral intervention practices as well as access to services (e.g., on-site nutritionist, diabetes education) could vary by clinic site. We also only assessed recommendation implementation for 18 months post-recommendation release and it is possible that the guideline may have taken longer to be fully implemented. However, given that most of the PCPs interviewed more than 3 years after recommendation release were still unaware of the guideline, we do not feel that extended quantitative follow-up would have yielded much different results. There were no plausible negative control variables or populations available to us to address potential residual confounding in the interrupted time-series analysis.22 Physicians who responded to interview requests may have had more interest in diabetes prevention than those who did not. We also only interviewed physicians but other team members or clinic staff such as nutritionists or diabetes educators have valuable input on diabetes screening and prediabetes treatment practices. Lastly, if physicians did not document diagnoses or referrals in the appropriate EHR fields, our estimates of clinician screening and referrals may be incorrect though it would likely be non-differential given limited awareness of the recommendations. Since this study’s health system did not have a formal referral process for intensive behavioral interventions, such as the Diabetes Prevention Program, the findings reported pertain to any behavioral intervention with a formal referral process in the EHR; to assess this limitation, we conducted a chart audit of PCP notes for 100 randomly selected patients from our sample and found no mention of referral to intensive behavioral interventions in chart text.
Implementation studies are vital in assessing the extent to which the implications of research findings are incorporated into usual care. More than 80% of US adults have annual visits with primary care providers.23 This makes PCPs a key mode for delivery of evidence-based diabetes prevention interventions by identifying patients with prediabetes, counseling them on behavioral changes, and referring them to intensive behavioral interventions. Our study results suggest significant opportunities to improve diabetes prevention efforts within health systems by (1) promoting awareness of USPSTF clinical recommendations and (2) implementing EHR modifications that both identify patients to be screened based on guideline recommendations and facilitate referral of those with prediabetes to intensive behavioral interventions. In this way, we have the potential to improve patient care and reduce diabetes incidence.
References
National Center for Chronic Disease Prevention and Health Promotion. National Diabetes Statistics Report, 2014 Estimates of Diabetes and Its Burden in the Epidemiologic Estimation Methods.; 2014.
Zimmermann LJ, Thompson JA, Persell SD. Electronic Health Record Identification of Prediabetes and an Assessment of Unmet Counselling Needs. J Eval Clin Pract. 2012;18(4):861-865. https://doi.org/10.1111/j.1365-2753.2011.01703.x
Schmittdiel JA, Adams SR, Segal J, et al. Novel Use and Utility of Integrated Electronic Health Records to Assess Rates of Prediabetes Recognition and Treatment: Brief Report from an Integrated Electronic Health Records Pilot Study. Diabetes Care. 2014;37(2):565-568. https://doi.org/10.2337/dc13-1223
Karve A, Hayward RA. Impaired Fasting Glucose and Impaired Glucose Tolerance in Nondiabetic U.S. Adults. Diabetes Care. 2010;33(11):2355-2359. https://doi.org/10.2337/dc09-1957.
Mainous AG, Tanner RJ, Baker R. Prediabetes Diagnosis and Treatment in Primary Care. J Am Board Fam Med. 2016;29(2):283-285. https://doi.org/10.3122/jabfm.2016.02.150252
Siu AL. Screening for Abnormal Blood Glucose and Type 2 Diabetes Mellitus: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163(11):861-868. https://doi.org/10.7326/M15-2345
Mickan S, Burls A, Glasziou P. Patterns of “Leakage” in the Utilisation of Clinical Guidelines: a Systematic Review. Postgrad Med J. 2011;87(1032):670-679. https://doi.org/10.1136/pgmj.2010.116012
Pathman DE, Konrad TR, Freed GL, Freeman V A, Koch GG. The Awareness-to-Adherence Model of the Steps to Clinical Guideline Compliance. The Case of Pediatric Vaccine Recommendations. Med Care. 1996;34(9):873-889. https://doi.org/10.1097/00005650-199609000-00002
Schoonenboom J, Johnson RB. How To Construct a Mixed Methods Research Design. Kolner Zeitschrift fur Soziol. 2017;69:107-131. https://doi.org/10.1007/s11577-017-0454-1
Creswell J, Plano Clark V. Choosing a mixed methods design. In: Designing and conducting mixed methods research. 2006:58-89.
Sandelowski M. Mixed method_ Focus on Research Methods Combining Qualitative and Quantitative Sampling, Data Collection, and Analysis Techniques in Mixed-Method Studies_XXX. Res Nurs Heal. 2000;23(3):246-255. http://onlinelibrary.wiley.com/doi/10.1002/1098-240X(200006)23:3%3C246::AID-NUR9%3E3.0.CO;2-H/pdf.
Shadish, William R., Thomas D. Cook and DTC. Experimental and Designs for Generalized Causal Inference.; 2002.
Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented Regression Analysis of Interrupted Time Series Studies in Medication Use Research. J Clin Pharm Ther. 2002;27(4):299-309. https://doi.org/10.1046/j.1365-2710.2002.00430.x
Kinlaw AC, Stürmer T, Lund JL, et al. Trends in Antibiotic Use by Birth Season and Birth Year. Pediatrics. 2017;140(3). https://doi.org/10.1542/peds.2017-0441
Stolwijk AM, Straatman H, Zielhuis GA. Studying seasonality by using sine and cosine functions in regression analysis. 1999:235-238.
Brookhart MA, Rothman KJ. Simple Estimators of the Intensity of Seasonal Occurrence. 2008;9:1-9. https://doi.org/10.1186/1471-2288-8-67
Hsieh H, Shannon SE. Three Approaches to Qualitative Content Analysis. Qual Health Res. 2005;15(9):1277-1288. https://doi.org/10.1177/1049732305276687
Mainous AG, Tanner RJ, Scuderi CB, Porter M, Carek PJ. Prediabetes Screening and Treatment in Diabetes Prevention: The Impact of Physician Attitudes. J Am Board Fam Med. 2016;29(6):663-671. https://doi.org/10.3122/jabfm.2016.06.160138
Tseng E, Greer RC, O’Rourke P, et al. Survey of Primary Care Providers’ Knowledge of Screening for, Diagnosing and Managing Prediabetes. J Gen Intern Med. 2017;32(11):1172-1178. https://doi.org/10.1007/s11606-017-4103-1
Nhim K, Khan T, Gruss SM, et al. Primary Care Providers’ Prediabetes Screening, Testing, and Referral Behaviors. Am J Prev Med. 2018;55(2):e39-e47. https://doi.org/10.1016/j.amepre.2018.04.017
Chambers EC, Wylie-Rosett J, Blank AE, et al. Increasing Referrals to a YMCA-Based Diabetes Prevention Program: Effects of Electronic Referral System Modification and Provider Education in Federally Qualified Health Centers. Prev Chronic Dis. 2015;12:1-7. https://doi.org/10.5888/pcd12.150294
Lipsitch, Marc; Tchetgen, Eric; Cohen T. Negative Controls: a Tool for Detecting Confounding and Bias in Observational Studies. Epidemiology. 2010;23(1):1-7. https://doi.org/10.1038/jid.2014.371
Phillips RL, Bazemore AW. Primary Care and Why It Matters for U.S. Health System Reform. Health Aff. 2010;29(5):806-810. https://doi.org/10.1377/hlthaff.2010.0020
Funding
This research was funded by the Agency for Healthcare Quality and Research, Grant No. 1 R36 HS025561-01A1 (Thomas).
This research was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489.
This research was also partially supported by a National Research Service Award Pre-Doctoral Traineeship (Thomas) and Post-Doctoral Fellowship (Kinlaw) from the Agency for Healthcare Research and Quality sponsored by the Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill, Grant No. 5T32 HS000032-28.
Dr. Thomas received funding from The Permanente Medical Group (TPMG) Delivery Science Fellowship Program and the National Institute of Diabetes and Digestive and Kidney Diseases grant T32DK11668401.
Dr. Golin’s salary was partially supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (5K24HD069204).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Thomas reports grants from the Agency for Healthcare Research and Quality, grants from the National Institute of Diabetes and Digestive and Kidney Diseases, and grants from the National Center for Advancing Translational Sciences, during the conduct of the study.
Dr. Golin reports grants from the Agency for Healthcare Research and Quality, during the conduct of the study; personal fees from iRT (innovation, Research, and Training, Inc.); and personal fees from UAMS ARCH-D Health Disparities Center, outside the submitted work.
Dr. Kinlaw reports grants from the Agency for Healthcare Research and Quality and grants from the National Center for Advancing Translational Sciences, during the conduct of the study.
Dr. Kirkman reports grans from Novo Nordisk, Bayer, outside the submitted work.
Dr. Golden has nothing to disclose.
Dr. Samuel-Hodge has nothing to disclose.
Dr. Lightfoot reports grants from the Agency for Healthcare Research and Quality and grants from the National Center for Advancing Translational Sciences, during the conduct of the study.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Thomas, T.W., Golin, C.E., Kinlaw, A.C. et al. Did the 2015 USPSTF Abnormal Blood Glucose Recommendations Change Clinician Attitudes or Behaviors? A Mixed-Method Assessment. J GEN INTERN MED 37, 15–22 (2022). https://doi.org/10.1007/s11606-021-06749-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-021-06749-x