
Abstract
Background
The antitumor effect of statins has been highlighted, but clinical study results remain inconclusive. While patients with diabetes are at high risk of cancer, it is uncertain whether statins are effective for cancer chemoprevention in this population.
Objective
This study evaluated the association between statins and cancer incidence/mortality in patients with type 2 diabetes.
Design
This study was a follow-up observational study of the Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) trial, which was a randomized controlled trial of low-dose aspirin in Japanese patients with type 2 diabetes.
Participants
This study enrolled 2536 patients with type 2 diabetes, age 30–85 years, and no history of atherosclerotic cardiovascular disease, from December 2002 until May 2005. All participants recruited in the JPAD trial were followed until the day of any fatal event or July 2015. We defined participants taking any statin at enrollment as the statin group (n = 650) and the remainder as the no-statin group (n = 1886).
Main Measures
The primary end point was the first occurrence of any cancer (cancer incidence). The secondary end point was death from any cancer (cancer mortality).
Key Results
During follow-up (median, 10.7 years), 318 participants developed a new cancer and 123 died as a result. Cancer incidence and mortality were 10.5 and 3.7 per 1000 person-years in the statin group, and 16.8 and 6.3 per 1000 person-years in the no-statin group, respectively. Statin use was associated with significantly reduced cancer incidence and mortality after adjustment for confounding factors (cancer incidence: adjusted hazard ratio [HR], 0.67; 95% CI, 0.49–0.90, P = 0.007; cancer mortality: adjusted HR, 0.60; 95% CI, 0.36–0.98, P = 0.04).
Conclusions
Statin use was associated with a reduced incidence and mortality of cancer in Japanese patients with type 2 diabetes.
Similar content being viewed by others


INTRODUCTION
Statins are the most commonly prescribed lipid-lowering drugs for dyslipidemia and the prevention of atherosclerotic cardiovascular disease (ASCVD).1 Many guidelines recommend statin use in patients at high risk of ASCVD,1, 2 including patients with diabetes.2, 3 Recently, the antitumor effect of statins has been highlighted by clinical and experimental studies,4,5,6,7 and several mechanisms underlying this effect have been investigated in experimental studies.6, 8 However, the results of clinical studies remain inconclusive.9,10,11
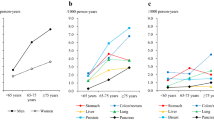
Accumulated evidence has demonstrated an interaction between diabetes and cancer.12,13,14,15 Several cancers, such as hepatic, colorectal, and pancreatic cancers, were reported to occur at a higher incidence in patients with diabetes than in those without.14, 15 In Japan, cancer is the leading cause of death not only in the general population but also in patients with diabetes. Notably, over one third of Japanese patients with diabetes die from cancer.16 These findings suggest that cancer prevention is necessary for improving the quality of life and prognosis of patients with diabetes.
In 2018, we reported the effect of low-dose aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes in the Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) 2 cohort study.17 The JPAD2 cohort study was a follow-up observational study of the JPAD trial, which was a randomized controlled trial (RCT) of low-dose aspirin for primary prevention of ASCVD in Japanese patients with type 2 diabetes.18, 19 The follow-up survey of the JPAD2 cohort is ongoing, with a median follow-up period of over 10 years at the time of this writing. By using the JPAD2 cohort, this study aimed to evaluate the association between statins and the incidence of cancer in Japanese patients with type 2 diabetes, a population that is at high risk of cancer.
METHODS
Study Design
The detailed design of the JPAD2 cohort study was previously described.17 In brief, the JPAD2 cohort study comprised the JPAD trial and its follow-up observational study. The JPAD trial was an RCT conducted in Japan to evaluate the effect of low-dose aspirin on the primary prevention of cardiovascular events in patients with type 2 diabetes (Clinicaltrials.gov: NCT00110448).18 Participants in the JPAD trial were enrolled from December 2002 until May 2005. After the JPAD trial was completed in April 2008, participants were administered low-dose aspirin according to the decision of each physician in charge. All participants were followed until the day of any fatal event or July 2015, whichever occurred first, even if cardiovascular events occurred. If participants were not followed up until July 2015, they were censored on the day of their last visit.
The JPAD trial and JPAD2 cohort study were performed according to the Declaration of Helsinki and were approved by the ethics committee of each participating hospital (Nara Medical University Ethics Committee and Graduate School of Medical Science, Kumamoto University Ethics Committee). Written informed consent was obtained from each participant.
Study Participants
The JPAD2 cohort study included 2536 Japanese patients with type 2 diabetes, age 30–85 years, and no history of ASCVD, who were recruited in the JPAD trial.17 The detailed inclusion and exclusion criteria of the JPAD trial were described previously.18 In the original JPAD trial, physicians in charge excluded the patients who had a history of clinically evident cancer, because they were inappropriate for long-term follow-up.
Exposure
Participants who were taking any statin at enrollment in the JPAD trial were defined as the statin group (n = 650), while those who were not taking a statin were defined as the no-statin group (n = 1886). The assignment of the statin/no-statin groups remained at baseline, even if there was a change in statin use during the follow-up period.
Primary and Secondary End Points
We defined the primary end point as the time to first occurrence of any cancer after the JPAD trial enrollment (cancer incidence). The secondary end point was death from any cancer (cancer mortality). Cancer incidence and mortality encompassed all types of malignant neoplasms. We collected data on cancer occurrence and death by contacting each physician in charge. The study secretariat asked them for detailed information on the cancers (i.e., onset date, site, and tissue type), and on deaths (date and cause of death). We excluded cancer events that occurred prior to enrollment and cancer events for which there was insufficient information. All potential end points were adjudicated by a central independent committee that was blinded to participants’ characteristics.
Statistical Analysis
Categorical variables were expressed as numbers and percentages, and were compared with the chi-square test. Continuous variables were expressed as means ± SDs or medians (interquartile range). Based on their distribution, continuous variables were compared using the Student’s t test or Wilcoxon rank sum test, as appropriate. Comparisons between the statin and no-statin groups were made on the basis of time to the first event, according to the intention-to-treat principle. Since the mortality from cardiovascular events was low in the JPAD2 cohort study and we followed all participants after these events, the cause-specific cumulative incidence of each end point was estimated using the Kaplan-Meier method in each group, and differences between groups were assessed with the log-rank test. We constructed multivariable Cox proportional hazard models to estimate the hazard ratio (HR) and 95% CI of the efficacy of statins in terms of the end point incidences. We adjusted for the following factors at baseline: age (≥ 65 or < 65 years), sex, body mass index (BMI), history of smoking status (current or past smoking), low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, hemoglobin A1c (HbA1c), allocation of low-dose aspirin, and administration of metformin, insulin, and thiazolidinedione. These factors were considered to affect the incidence of cancer events in previous studies.14, 17, 20,21,22,23,24 In these models, BMI, LDL cholesterol, HDL cholesterol, and HbA1c were dichotomized by median values of 24 kg/m2, 119 mg/dL, 53 mg/dL, and 7.2%, respectively, to fulfill the proportional hazard assumptions for Cox models. The LDL cholesterol level was calculated by the Friedewald formula.
In subgroup analyses, we stratified the participants by age, sex, BMI, smoking status, LDL cholesterol, HDL cholesterol, and HbA1c. In each subgroup, we used the same multivariable Cox proportional hazard models to assess the efficacy of statins on cancer incidence.
As sensitivity analyses, we excluded data from the first 3 years after enrollment in the JPAD trial when analyzing the effect of statins on cancer incidence, to ensure that we did not include any undiagnosed cancers at enrollment. To evaluate patients who started statins during the follow-up period, we performed sensitivity analyses with the addition of patients who were newly prescribed statins in 2009, as the statin group.
Statistical analyses were conducted by an independent statistician (T.M.) with the use of JMP 12.2 (SAS Institute, Cary, NC) and SAS 9.4 (SAS Institute, Cary, NC). Two-tailed P values less than 0.05 were considered statistically significant.
RESULTS
Characteristics of Patients in the Statin and No-Statin Groups at Baseline
At the time of enrollment in the JPAD trial, 650 (26%) participants were taking a statin. Baseline characteristics stratified by statin use are presented in Table 1. The proportion of male participants was 36% in the statin group and 61% in the no-statin group, indicating that many of the participants taking statins were female. The smoking rate was significantly higher in the no-statin group (current: 15% vs. 23%, P < 0.0001; past: 16% vs. 22%, P = 0.002). The statin group showed higher serum levels of total cholesterol, fasting triglyceride, and HDL cholesterol than the non-statin group, but the LDL cholesterol level was the same in both groups. In terms of antihyperglycemic medications, the frequency of sulfonylurea use was higher in the statin group (61% vs. 56%, P = 0.02), that of insulin was higher in the no-statin group (9% vs. 14%, P = 0.001), and those of metformin and thiazolidinedione were similar in both groups (metformin: 14% vs. 14%, P = 0.8; thiazolidinedione: 6% vs. 5%, P = 0.2). Low-dose aspirin had been randomly assigned in both groups by the JPAD trial (50% vs. 50%, P = 0.9).
Association Between Statin Use and Cancer Incidence
As of July 2015, we had followed the participants for a median of 10.7 (95% CI, 10.5–10.8) years. During the follow-up period, 318 cancer events occurred: 58 (10.5 per 1000 person-years) in the statin group and 260 (16.8 per 1000 person-years) in the no-statin group. The details of each cancer incidence are shown in Table 2. Kaplan-Meier curves showed that statin use was associated with significantly reduced cancer incidence (log-rank, P < 0.001; HR, 0.62; 95% CI, 0.46–0.81, P < 0.001; Fig. 1a). Multivariable Cox hazard models indicated that statin use was associated with significantly reduced cancer incidence after adjusting for other related factors (adjusted HR, 0.67; 95% CI, 0.49–0.90; P = 0.007). We did not analyze the effect of statins by cancer type, because the total number of cancers in our study precluded an analysis by cancer type (Table 2).

Association between statin use and cancer incidence/mortality. Kaplan-Meier estimates show the association between statin use and cancer incidence (a) / cancer mortality (b). These estimates were not adjusted for baseline characteristics. Both the crude HR and that obtained via multivariable analysis are presented. The multivariable analysis was adjusted for age, sex, BMI, smoking status, LDL cholesterol, HDL cholesterol, HbA1c, allocation of low-dose aspirin, and administration of metformin, insulin, and thiazolidinedione. HR, hazard ratio; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, hemoglobin A1c.
Many subgroups of the statin group had a consistently lower incidence of cancer, but several subgroups did not show any benefit of statins (Fig. 2). In particular, in the subgroup with lower LDL cholesterol, statin use was associated with significantly reduced cancer incidence (adjusted HR, 0.48; 95% CI, 0.30–0.74; P < 0.001); however, this was not the case in the subgroup with higher LDL cholesterol (adjusted HR, 0.95; 95% CI, 0.62–1.43; P = 0.8; interaction, P = 0.03).

Subgroup analyses of effects of statin use on cancer incidence stratified by baseline characteristics. These plots show effects of statin use on cancer incidence in subgroups stratified by baseline characteristics. HRs were adjusted for age, sex, BMI, smoking status, LDL cholesterol, HDL cholesterol, HbA1c, allocation of low-dose aspirin, and administration of metformin, insulin, and thiazolidinedione. HR, hazard ratio; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, hemoglobin A1c.
To ensure that we did not include any undiagnosed cancers at enrollment, we excluded data from the first 3 years after enrollment in the JPAD trial. In the first 3 years, 68 participants developed cancer; after excluding that 3-year period, statin use was still associated with significantly reduced cancer incidence (log-rank, P = 0.006; HR, 0.65; 95% CI, 0.47–0.88; P = 0.005). The multivariable Cox hazard model showed that statins still reduced cancer incidence but nonsignificantly so (adjusted HR, 0.73; 95% CI, 0.52–1.02; P = 0.06).
In 2009, 272 participants in the no-statin group newly took statins. In sensitivity analyses with the addition of patients who were newly prescribed statins, statin use was still associated with significantly reduced cancer incidence (adjusted HR, 0.56; 95% CI, 0.42–0.73; P < 0.0001).
Association Between Statin Use and Cancer Mortality
Sixty-six participants in the statin group died, 21 from cancer (3.7 per 1000 person-years). Two hundred sixty-five participants in the no-statin group died, 102 from cancer (6.3 per 1000 person-years). Cancer was the leading cause of death both in the statin and no-statin groups (Table 3). Survival analyses showed that statin use was associated with significantly reduced cancer mortality (log-rank, P = 0.02; HR, 0.58; 95% CI, 0.35–0.90; P = 0.02; Fig. 1b). Multivariable Cox hazard models also showed a significant difference between groups (adjusted HR, 0.60; 95% CI, 0.36–0.98; P = 0.04).
DISCUSSION
This study showed that statin use was associated with significantly reduced cancer incidence and mortality, after adjusting for potentially confounding factors. Most subgroup analyses showed consistent results. The results were also robust after multiple sensitivity analyses.
Previous clinical trials demonstrated controversial results regarding the efficacy of statins in cancer chemoprevention. Many RCTs of statins have been conducted to examine ASCVD prevention, and meta-analyses using these RCTs to evaluate cancer chemoprevention showed negative results.5, 9 The observational periods were less than 5 years in most of these RCTs, and because carcinogenesis is a long-term process, this duration may be too short to assess cancer chemoprevention. On the other hand, long-term cohort studies have demonstrated positive results regarding statins and cancer chemoprevention.4, 11 With a median follow-up period of 10.7 years, our study was able to evaluate the association between statins and cancer incidence, despite the small number of participants.
Because this study is a follow-up cohort study of an RCT investigating low-dose aspirin, there were significant differences in baseline characteristics between the statin and no-statin groups. For instance, the smoking rate was significantly lower in the statin group (Table 1), and smoking strongly affects the incidence of various cancers.20 Since statins are used preventively for ASCVD, it is possible that the participants who were taking statins were more interested in or informed about health issues. ASCVD and cancer share risk factors, and cancer occurrence, might be reduced in people who are proactive regarding risk control (so-called healthy user bias). However, our findings demonstrated that statin use was associated with significantly reduced cancer incidence and mortality, even after adjusting for as many confounding factors as possible, including smoking status. In fact, a subgroup analysis showed that statin use was associated with reduced cancer incidence rather in the current or past smoking group (Fig. 2).
LDL cholesterol levels were the same between the statin and no-statin groups, but total cholesterol levels were lower in the no-statin group (Table 1). These findings indicated that the participants in the no-statin group originally had lower serum cholesterol levels. Several studies reported an association between cancer occurrence and lower serum cholesterol levels.25,26,27,28 Cancer progression activates cholesterol metabolism even in the subclinical period, and decreases serum cholesterol levels.29, 30 In our study, cancer incidence was higher in participants with lower LDL cholesterol (LDL cholesterol < 119 mg/dL: 16.7 per 1000 person-years; LDL cholesterol ≥ 119 mg/dL: 13.2 per 1000 person-years). Based on these facts, the risk of cancer in the no-statin group might be essentially higher than that in the statin group. Thus, we adjusted the LDL cholesterol level to assess the association between statin use and incidence of cancer. We also analyzed the effect of statins on cancer incidence after excluding the first 3 years of the study period to eliminate undiagnosed cancers at enrollment. These analyses produced similar results.
The subgroup with lower LDL cholesterol showed an association between statin use and low cancer incidence, whereas the subgroup with higher LDL cholesterol did not (Fig. 2). There were several possible reasons for the difference of statins’ effect in the subgroups of LDL cholesterol. First, the patients with lower LDL cholesterol had originally high cancer risk,25,26,27 and the effect of statins on cancer chemoprevention in the patients with lower LDL cholesterol might be more easily detected than those in patients with higher LDL cholesterol. Next, cancer risk might be low in the statin user of the subgroup with lower LDL cholesterol, because their original LDL cholesterol level was considered to be higher if they did not take statins. Similar findings were observed in a previous study from the Hong Kong Diabetes Registry. This study reported that the use of statins on cancer chemoprevention was more effective in patients with lower LDL cholesterol and elevated albuminuria than those without.31 They hypothesized the mechanisms that low LDL cholesterol might upregulate the mevalonate pathway to lead carcinogenesis28; however, there remains insufficient evidence.
Several hypotheses have been proposed for the antitumor effects of statins in experimental studies. The inhibition of the mevalonate pathway by statins and the reduction of its downstream products necessary to maintain cellular functions are thought to decrease proliferation and migration of cancer cells.10, 32 An association between increased cancer risk in diabetes and cholesterol metabolism has also been investigated. One of the hypotheses is that increased insulin-like growth factor 1 signal in diabetes activates the mevalonate pathway via sterol regulatory element-binding protein and promotes cancer risk.33 This hypothesis predicts that statins might be more effective for cancer chemoprevention in patients with diabetes, but further investigation is needed to reveal them.
This study had several limitations. First, our study design could not cope with several biases on the cohort study: prevalent user bias, drug use indication bias, and immortal time bias.34 However, our study aimed to evaluate the difference between statin use in clinical practice and cancer incidence. Therefore, we analyzed the association between baseline use of statins and cancer incidence, adjusted for confounding factors related to cancer occurrence. Second, there was no data on the levels of serum lipid at the time before taking statin. Serum lipid levels were reported to indicate cancer risk,28 but the baseline levels of serum lipid were affected by taking statin in the statin group and were not considered to reflect cancer risk. As a second-best measure, we conducted the multivariable analyses for adjusting serum cholesterol levels at baseline, and the subgroup analyses stratified by baseline cholesterol levels. Third, we did not analyze the effect of statins by cancer type. Although it is important to examine if statin therapy has a beneficial effect on specific cancers, the total number of cancers in our study precluded an analysis by cancer type. This important clinical question should be investigated in future studies when additional data are available. Fourth, previous reports suggested that lipophilic statins were more effective for cancer chemoprevention than hydrophilic statins.10 However, we did not collect information regarding different statin agents in the present study. Fifth, we had no data regarding each participant’s adherence with statin treatment. However, if there was low adherence with statin use in the statin group, the fact should weaken the association between statin use and cancer incidence in analyses. Therefore, the positive association in the current analyses should be considered robust.
In conclusion, since carcinogenesis is a long-term process, it needs long-term follow-up to assess cancer chemoprevention. Over 10-year follow-up of the JPAD2 cohort study suggested that statin use was beneficial for cancer chemoprevention in patients with type 2 diabetes. Statins should be originally prescribed for lowering serum lipid levels to prevent ASCVD in patients with diabetes, but they might also have an effect of cancer chemoprevention in long-term use. Realistically, it is difficult to conduct an RCT to analyze the effect of statins on cancer risk, and accumulation of clinical observational data should lead to clarify the relationship between statins and cancer in patients with diabetes.
References
Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;139:e1082-e1143.
Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016;37:2315-2381.
American Diabetes Association. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2019. Diabetes Care. 2019;42:S103-S123.
Nielsen SF, Nordestgaard BG, Bojesen SE. Statin use and reduced cancer-related mortality. N Engl J Med 2012;367:1792-1802.
Kim MK, Myung SK, Tran BT, Park B. Statins and risk of cancer: a meta-analysis of randomized, double-blind, placebo-controlled trials. Indian J Cancer 2017;54:470-477.
Sopkova J, Vidomanova E, Strnadel J, Skovierova H, Halasova E. The role of statins as therapeutic agents in cancer. Gen Physiol Biophys 2017;36:501-511.
Ahmadi Y, Karimian R, Panahi Y. Effects of statins on the chemoresistance-the antagonistic drug-drug interactions versus the anti-cancer effects. Biomed Pharmacother 2018;108:1856-1865.
Altwairgi AK. Statins are potential anticancerous agents (review). Oncol Rep 2015;33:1019-1039.
Cholesterol Treatment Trialists C, Emberson JR, Kearney PM, et al. Lack of effect of lowering LDL cholesterol on cancer: meta-analysis of individual data from 175,000 people in 27 randomised trials of statin therapy. PLoS One. 2012;7:e29849.
May MB, Glode A. Novel uses for lipid-lowering agents. J Adv Pract Oncol 2016;7:181-187.
Wang A, Aragaki AK, Tang JY, et al. Statin use and all-cancer survival: prospective results from the Women’s Health Initiative. Br J Cancer 2016;115:129-135.
Giovannucci E, Harlan DM, Archer MC, et al. Diabetes and cancer: a consensus report. Diabetes Care 2010;33:1674-1685.
Noto H, Osame K, Sasazuki T, Noda M. Substantially increased risk of cancer in patients with diabetes mellitus: a systematic review and meta-analysis of epidemiologic evidence in Japan. J Diabetes Complications 2010;24:345-353.
Emerging Risk Factors C, Seshasai SR, Kaptoge S, et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364:829-841.
Kasuga M, Ueki K, Tajima N, et al. Report of the JDS/JCA Joint Committee on Diabetes and Cancer. Diabetology International 2013;4:81-96.
Nakamura J, Kamiya H, Haneda M, et al. Causes of death in Japanese patients with diabetes based on the results of a survey of 45,708 cases during 2001-2010: report of the Committee on Causes of Death in Diabetes Mellitus. J Diabetes Investig 2017;8:397-410.
Okada S, Morimoto T, Ogawa H, et al. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care 2018;41:1757-1764.
Ogawa H, Nakayama M, Morimoto T, et al. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA 2008;300:2134-2141.
Saito Y, Okada S, Ogawa H, et al. Low-dose aspirin for primary prevention of cardiovascular events in patients with type 2 diabetes mellitus: 10-year follow-up of a randomized controlled trial. Circulation 2017;135:659-670.
Sasco AJ, Secretan MB, Straif K. Tobacco smoking and cancer: a brief review of recent epidemiological evidence. Lung Cancer 2004;45 Suppl 2:S3-9.
Zhao W, Guan J, Horswell R, et al. HDL cholesterol and cancer risk among patients with type 2 diabetes. Diabetes Care 2014;37:3196-3203.
Gallagher EJ, LeRoith D. Obesity and diabetes: the increased risk of cancer and cancer-related mortality. Physiol Rev 2015;95:727-748.
Coyle C, Cafferty FH, Vale C, Langley RE. Metformin as an adjuvant treatment for cancer: a systematic review and meta-analysis. Ann Oncol 2016;27:2184-2195.
Ripamonti E, Azoulay L, Abrahamowicz M, Platt RW, Suissa S. A systematic review of observational studies of the association between pioglitazone use and bladder cancer. Diabet Med 2019;36:22-35.
Asano K, Kubo M, Yonemoto K, et al. Impact of serum total cholesterol on the incidence of gastric cancer in a population-based prospective study: the Hisayama study. Int J Cancer 2008;122:909-914.
Iso H, Ikeda A, Inoue M, Sato S, Tsugane S, Group JS. Serum cholesterol levels in relation to the incidence of cancer: the JPHC study cohorts. Int J Cancer 2009;125:2679-2686.
Nago N, Ishikawa S, Goto T, Kayaba K. Low cholesterol is associated with mortality from stroke, heart disease, and cancer: the Jichi Medical School Cohort Study. J Epidemiol 2011;21:67-74.
Yang X, So W, Ko GT, et al. Independent associations between low-density lipoprotein cholesterol and cancer among patients with type 2 diabetes mellitus. CMAJ 2008;179:427-437.
Kuzu OF, Noory MA, Robertson GP. The role of cholesterol in cancer. Cancer Res 2016;76:2063-2070.
Murai T. Cholesterol lowering: role in cancer prevention and treatment. Biol Chem. 2015;396:1-11.
Yang X, So WY, Ma RC, et al. Low LDL cholesterol, albuminuria, and statins for the risk of cancer in type 2 diabetes: the Hong Kong diabetes registry. Diabetes Care 2009;32:1826-1832.
Iannelli F, Lombardi R, Milone MR, et al. Targeting mevalonate pathway in cancer treatment: repurposing of statins. Recent Pat Anticancer Drug Discov 2018;13:184-200.
Yang X, Lee HM, Chan JC. Drug-subphenotype interactions for cancer in type 2 diabetes mellitus. Nat Rev Endocrinol 2015;11:372-379.
Yang XL, Ma RC, So WY, Kong AP, Xu G, Chan JC. Addressing different biases in analysing drug use on cancer risk in diabetes in non-clinical trial settings--what, why and how? Diabetes Obes Metab 2012;14:579-585.
Acknowledgments
The authors thank M. Ohtorii for her roles in data management and statistical analyses. The authors also thank M. Nagahiro, M. Okamoto, and M. Aoyama, and Y. Wada, Y. Kamada, and M. Miyagawa for their secretarial work. The authors also thank all members of the JPAD trial investigators, described in the Appendix, for data collection.
This study was supported by the Ministry of Health, Labour and Welfare of Japan (H16-Junkanki-004, and H27-Junkanki-Ippan-001), the Japan Heart Foundation, and JSPS KAKENHI Grant Number 17K18022.
This study has not been presented at any conference.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Okada reports personal fees from Novo Nordisk, Mitsubishi Tanabe, Sumitomo Dainippon, Arkray, Bayer, Eli Lilly, Boehringer Ingelheim, Ono, AstraZeneca, Sanofi, and Takeda, outside the submitted work. Dr. Morimoto reports personal fees from AstraZeneca, Bayer, Daiichi Sankyo, Japan Lifeline, Kyocera, Mitsubishi Tanabe, Novartis, Pfizer, Asahi Kasei, Bristol-Myers Squibb, and Boston Scientific, outside the submitted work. Dr. Ogawa reports personal fees from MSD, Daiichi Sankyo, Ono, Mochida, AstraZeneca, Pfizer, Bristol-Myers Squibb, Mitsubishi Tanabe, Kyowa Kirin, Sanofi, and Medtronic, outside the submitted work. Dr. Soejima reports grants from Boehringer Ingelheim, outside the submitted work. Dr. Matsumoto has nothing to disclose. Dr. Sakuma reports personal fees from Enomoto Pharmaceutical, outside the submitted work. Dr. Nakayama reports personal fees from Bayer, Shionogi, Takeda, Daiichi Sankyo, Sanofi, Boehringer Ingelheim, Sumitomo Dainippon, Fujifilm Medical, Kowa, Pfizer, and Astellas, outside the submitted work. Dr. Doi reports personal fees from Daiichi Sankyo, Mitsubishi Tanabe, Takeda, Otsuka, Astellas, Boehringer Ingelheim, Abbott, Bayer, Medtronic, Pfizer, Kowa, MSD, and Actelion, outside the submitted work. Dr. Jinnouchi reports grants and personal fees from MSD, Boehringer Ingelheim, Novo Nordisk, Daiichi Sankyo, Takeda, Taisho Toyama, Astellas, Bayer, Sanofi, Sanwa Kagaku Kenkyusho, Eli Lilly, AstraZeneca; grants from Chugai, GlaxoSmithKline, Ono, Pfizer, Shionogi; personal fees from Abbott, Terumo, Kyowa Kirin, Teijin, Mitsubishi Tanabe, outside the submitted work. Dr. Waki reports grants and personal fees from Sanofi, AstraZeneca; personal fees from MSD, Astellas, Amgen Astellas BioPharma, Otsuka, Ono, Kowa, Kyowa Kirin, Novartis, Sanwa Kagaku Kenkyusho, Johnson & Johnson, Daiichi Sankyo, Taisho Toyama, Sumitomo Dainippon, Takeda, Mitsubishi Tanabe, Teijin, Eli Lilly, Novo Nordisk, Bayer, Pfizer, Boehringer Ingelheim, Abbott, outside the submitted work. Dr. Masuda reports personal fees from AstraZeneca, Ono, Takeda, Astellas, Bayer, Boehringer Ingelheim, Eli Lilly, Daiichi Sankyo, Kowa, Kyowa Kirin, MSD, Novartis, Shionogi, Mitsubishi Tanabe, outside the submitted work. Dr. Saito reports grants and personal fees from Bayer, Otsuka, Novartis, Ono, Mitsubishi Tanabe, Astellas, Asahi Kasei, Daiichi Sankyo, Sumitomo Dainippon, Fuji Yakuhin, Kowa, Kyowa Kirin, MSD, Sanofi, Takeda; grants from Terumo, Amgen Astellas BioPharma, Shionogi, Teijin, St. Jude Medical, Actelion, Boston Scientific, Chugai, Eisai, Medtronic, Nihon Medi-Physics, Zeria; personal fees from Boehringer Ingelheim, Pfizer, Taisho Toyama, Toa Eiyo, outside the submitted work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 37.6 kb)
Rights and permissions
About this article

Cite this article
Okada, S., Morimoto, T., Ogawa, H. et al. Association Between Statins and Cancer Incidence in Diabetes: a Cohort Study of Japanese Patients with Type 2 Diabetes. J GEN INTERN MED 36, 632–639 (2021). https://doi.org/10.1007/s11606-020-06167-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-020-06167-5