
Abstract
Background
Numerous studies have examined if food insecurity (FI) leads to increased weight gain, but little is known about how FI affects obese participants.
Objective
Our objective was to determine if obese, food-insecure adults are more likely to have medical comorbidities than obese, food-secure adults.
Design
We conducted a cross-sectional study using the 2007–2014 National Health and Nutrition Examination Survey (NHANES).
Participants
All obese participants (≥ 20 years) in NHANES were eligible. Participants who were pregnant or missing FI data were excluded.
Main Measures
The primary exposure was household FI, and the primary outcome was the total number of obesity-related comorbidities. Secondary outcomes evaluated the association between FI and individual comorbidities. Propensity score weighting was used to improve covariate balance. We used negative binomial regression to test the association between FI and the total number of comorbidities. We used logistic regression to test the association between FI and individual comorbidities.
Key Results
Of the 9203 obese participants, 15.6% were food insecure. FI (β = 0.09, 95% CI: 0.02, 0.15; p = 0.01) and very low food security (β = 0.17, 95% CI: 0.07, 0.28; p = 0.003) were associated with an increased number of comorbidities. In secondary analyses, FI was associated with increased odds of coronary artery disease (OR: 1.5, 95% CI: 1.1, 2.0) and asthma (OR: 1.3, 95% CI: 1.1, 1.6). Very low food security was associated with increased odds of coronary artery disease, diabetes, and asthma.
Conclusion
Obese adults living in food-insecure households were more likely to have an increased number of comorbid conditions than obese adults living in food-secure households. Clinicians should be aware of the association between FI and comorbid medical conditions when treating patients with obesity.
Similar content being viewed by others


INTRODUCTION
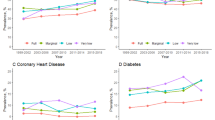
The social determinants of health (SDH), or the circumstances in which people are born, live, and age, have a profound influence on morbidity and mortality.1,2,3,4,5,6,7,8 Food insecurity (FI), the lack of consistent access to enough food, is an important SDH affecting 40 million Americans.9 FI is assessed by the US Department of Agriculture (USDA). Households are identified as having high food security (no indications of food access problems), marginal food security (anxiety over food sufficiency), low food security (individuals reduce the quality of their diet, but not food intake), and very low food security (multiple indications of disrupted eating patterns and reduced food intake).9
A growing body of research has found that FI is associated with negative health outcomes.10,11,12,13,14,15,16,17 Prior studies have also evaluated if FI is associated with obesity.18,19,20,21 Individuals living in food-insecure households are more likely to consume cheap, high-calorie foods and are less likely to be physically active, potentially leading to increased weight gain and obesity.22,23,24,25 Although prior studies have evaluated if FI leads to obesity, there is limited data about how FI affects individuals who are obese. Obese adults who are food insecure may have difficulty making lifestyle modifications due to limited resources. This difficulty in making lifestyle modifications could lead to obesity-related comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
Although prior studies have found that FI is associated with increased risk of cardiovascular risk factors in the general population,12,13,17 there is limited data assessing if FI is associated with chronic conditions among obese adults. To fill this gap in the literature, we evaluated if FI was associated with an increased number of comorbid conditions among obese adults. We hypothesized that adults who are obese and food insecure would be more likely to have an increased number of medical comorbidities than obese, food-secure individuals.
METHODS
Study Design and Data Sources
We conducted a cross-sectional analysis of data from the National Health and Nutrition Examination Survey (NHANES). NHANES is a series of large, cross-sectional surveys conducted by the National Center for Health Statistics.26 The data obtained in NHANES includes responses to an in-home interview on a variety of demographic and health characteristics, findings from a physical examination conducted at a mobile examination center, and laboratory measurements. NHANES is conducted in 2-year cycles, and we combined data from the 2007–2008, 2009–2010, 2011–2012, and 2013–2014 waves of NHANES. Further details of the study design and procedures have been previously published.26
Study Sample
We included all obese participants who were 20 years of age or older. Obesity is defined as a body mass index (BMI) ≥ 30. BMI was based on measured heights and weights from the NHANES examination. Participants who were pregnant (N = 93) or missing food insecurity data (N = 118) were excluded for a total unweighted sample size of 9203.
Exposure
The exposure of interest was household FI. FI was measured in NHANES using the 10-item Food Security Scale (https://www.ers.usda.gov/media/8279/ad2012.pdf).27 This validated questionnaire was developed by the USDA to measure household FI over the prior 12 months. NHANES administers the Food Security Scale in accordance with the USDA recommendations and uses the established scoring system for response to the items to categorize household food security: high food security (0 affirmative responses), marginal food security (1–2 affirmative responses), low food security (3–5 affirmative responses), and very low food security (6–10 affirmative responses).27 Consistent with USDA definitions, adults who report low or very low food security are considered to have FI.9 In this study, we analyzed the data using both the categorical FI variable (high food security, marginal food security, low food security, and very low food security) and FI as a binary variable by categorizing participants as food secure (0–2 affirmative responses) or food insecure (≥ 3 affirmative responses).9,12,28
Outcomes
The primary outcome was the total number of obesity-related medical comorbidities, a commonly used measure of multiple comorbid conditions.29,30 We included coronary artery disease, diabetes, hypertension, dyslipidemia, congestive heart failure, stroke, asthma, and obesity-associated cancers. Given some of these diseases may not constitute equivalent risk, secondary outcomes evaluated the association between FI and individual obesity-related comorbidities. Consistent with prior studies,10, 28 a participant was defined as having diabetes if they had any of the following: self-report of diabetes, a fasting glucose > 126, a glycolated hemoglobin > 6.5%, or currently taking a diabetic medication (including a sulfonylurea, insulin, or an incretin mimetic). A participant was defined as having dyslipidemia if they had any of the following: self-report of high cholesterol, currently taking a cholesterol lowering medication, or laboratory diagnosis for dyslipidemia (total ≥ 240 mg/dl, HDL < 30 mg/dl, LDL ≥ 160 mg/dl, triglycerides ≥ 150 mg/dl). Hypertension was defined as any of the following: self-report of high blood pressure, currently taking blood pressure medication, or elevated blood pressure based on the average of 3 blood pressure readings (systolic blood pressure > 140 mmHg or diastolic blood pressure > 90 mmHg).
Coronary artery disease was defined by self-report of a history of coronary artery disease, angina, or prior myocardial infarction. Congestive heart failure, stroke, and asthma were also based on self-report. Based on prior studies,31 a participant was defined as having any obesity-associated cancer (yes or no) if she or he reported any of the following: esophageal, stomach, liver, kidney, pancreatic, colon, rectal, gallbladder, breast, ovarian, or thyroid cancer.
Covariates
Covariates included demographic and clinical characteristics that have been associated with FI and/or obesity in prior studies.9,32 These included age, gender, and race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, or other). We included the household income-to-poverty ratio, highest education level achieved, current marital status, and if a participant reported being born outside of the USA. We further included participant’s BMI, smoking status (current, former, or never), health insurance (private, Medicare, public not including Medicare, or none), and if a participant reported using a nutrition assistance program (Supplemental Nutrition Assistance Program (SNAP), Special Supplemental Nutrition Assistance Program for Women, Children, and Infants (WIC), or received food from a food pantry or soup kitchen).
Statistical Analysis
Analyses were completed using Stata 15.0 (StataCorp, College Station, TX) and R Software (version 3.4.1).33 Participant characteristics were presented as mean (standard deviation) for continuous variables or N (percent) for categorical variables, and were compared using t tests and binomial tests. p values of < 0.05 were considered statistically significant. We used propensity score weighting to improve covariate balance between food-insecure and food-secure participants and potentially reduce estimate bias in complex survey data.34,35,36 We also ran multivariable regression models and found similar results to propensity models (online Supplemental Table 1). Propensity scores for food-secure vs food-insecure were estimated based on demographic and clinical covariates using a machine-learning technique called random forest using the R package randomForest.37,38 We used missForest imputation to replace missing values for income-to-poverty ratio (7.9% missing) and BMI (11.6% missing) in analysis estimating propensity scores. For the primary outcome, we used negative binomial regression to test the association between FI and total number of medical comorbidities. As a sensitivity analysis, we evaluated the association between FI and the total number of objectively measured comorbidities (diabetes, dyslipidemia, and hypertension) (online). We conducted stratified analyses by gender, age (which was included as a continuous variable in primary analyses but categorized as 20–45 years of age, 45–65 years of age, and > 65 years of age for stratified analysis only), and race/ethnicity to further evaluate relationships (online). For secondary outcomes, we used logistic regression to test the associations between FI and each individual comorbidity. All analyses were adjusted for the complex survey design of NHANES by applying sample weights, clustering, and the primary sampling unit. The Wake Forest School of Medicine Institutional Review Board deemed this study of publically available, de-identified data exempt from human subjects research.
RESULTS
Study Population Characteristics
Of the 9203 participants (weighted study population N = 333,135,322), the majority was female, non-Hispanic white, and had greater than a high school education level (Table 1). The mean age was 48.5 years (SD = 16.1 years) and the mean BMI was 35.9 (SD = 5.8). Of the participants, 15.6% lived in a food-insecure household, which included 9.0% with low food security and 6.6% with very low food security.
In bivariate analysis, FI was associated with younger age, lower educational attainment, lower household income-to-poverty ratio, lack of health insurance, and smoking (all p < 0.0001; Table 2). In unadjusted models, participants who were food insecure, compared with participants who were food secure, were more likely to report having ever received SNAP (58.3% vs 18.6%, p < 0.0001), receiving WIC in the last 12 months (17.1% vs 6.2%, p < 0.0001), and having used emergency food resources (food pantry, soup kitchen, or food bank) in the last 12 months (33.2% vs 3.9%, p < 0.0001). Food-insecure participants also had a significantly higher BMI than food-secure participants (36.9 vs 35.7, p < 0.0001).
Food Insecurity and Total Number of Obesity-Related Comorbid Conditions
In unadjusted analyses, participants in food-insecure households had a mean number of 1.73 (SD = 1.41) comorbid conditions while food-secure participants had a mean number of 1.66 (SD = 1.30) conditions. The propensity score model showed good model fit with FI as the dependent variable and all covariates included as the independent variables (C-statistic: 0.856; 95% CI: 0.848, 0.863, online Supplemental Figure 1). In propensity score weighted models, food-insecure adults had a significant increase in the total number of obesity-related comorbidities (β = 0.09, 95% CI: 0.02, 0.15; p = 0.01; Table 3). This was primarily seen among participants who lived in very low food-secure households (β = 0.17, 95% CI: 0.07, 0.28; p = 0.003). In sensitivity analyses evaluating the association between FI and total number of objectively measured comorbidities (diabetes, dyslipidemia, and hypertension), very low food security was also associated with an increased number of comorbidities (β = 0.12, 95% CI: 0.02, 0.21; p = 0.02; online Supplemental Table 2). Stratified analyses by gender and age found similar increases in comorbidities among adults in very low food-secure households (see online supplemental tables). Adults in very low food-secure households had an increase in the number of comorbidities within racial/ethnic groups, but the increase was only significant among non-Hispanic, Whites.
Food Insecurity and Individual Obesity-Related Comorbid Conditions
Our secondary outcomes were the association between FI and each obesity-related comorbidity (Table 4). FI was significantly associated with coronary artery disease (OR: 1.5; 95% CI: 1.1, 2.0, p = 0.01) and asthma (OR: 1.3; 95% CI: 1.1, 1.6, p = 0.002). The increased odds of coronary artery disease (OR: 2.0; 95% CI: 1.3, 3.0, p = 0.001) and asthma (OR: 1.5; 95% CI: 1.1, 2.0, p = 0.006) were primarily seen among participants living in very low food security households. Adults living in very low food security households also had significantly higher odds of diabetes (OR: 1.3; 95% CI: 1.1, 1.7, p = 0.02).
DISCUSSION
In this nationally representative sample, we found that obese, food-insecure adults were significantly more likely to have medical comorbidities than obese adults who were food secure. This was primarily seen among adults who lived in households with very low food security, and individuals living in a very low food security household were significantly more likely to have coronary artery disease, diabetes, and asthma. This data suggests that FI is associated with an increased prevalence of comorbid health conditions in obese adults.
Our results are consistent with the growing body of research showing FI is associated with an increased risk of chronic health conditions, including diabetes and other cardiovascular risk factors.10,11,12,13, 16, 28 Recently, a national study conducted by the USDA showed that FI is associated with an increased risk of ten common chronic conditions in non-elderly adults, including coronary artery disease, hypertension, and diabetes.16 Similar to our study, the authors found that households with the most severe form of FI, very low food security, were more likely to report these conditions. Our results add to this growing body of research by showing that FI is associated with an increased number of chronic conditions among obese adults, a group at increased risk of developing cardiovascular risk factors due to weight.
Prior studies have also evaluated if FI leads to an increased risk of weight gain and obesity.18,19,20,21 Compared with individuals in food-secure households, individuals living in food-insecure households are more likely to consume fewer fruits and vegetables, have higher intake of high-calories foods, and are less likely to be physically active.22,23,24,25 These behaviors could lead to increased weight gain and obesity, but also make it more difficult for obese adults to lose weight placing them at risk of developing comorbid conditions.
The causal mechanism by which FI leads to poor health outcomes remains unclear, but previous studies have hypothesized several pathways by which FI could lead to the development of chronic health conditions.39 These pathways include a nutrition pathway, characterized by deficits in the quality of food individuals eat; a mental health pathway, characterized by increased stress and depression due to concerns about having access to enough food; and a behavioral pathway, characterized by delays in seeking necessary medical care and obtaining prescribed medications because of concerns about cost.11,19,39,40,41,42,43,44,45 All of these pathways could contribute to the development or worsening of chronic health conditions. Understanding the relationship between these pathways and determining how to most effectively address the factors along these pathways in order to mitigate the negative health effects of FI should be a focus for future research.
Given our study was cross sectional, it is also possible that an increased number of comorbid conditions increases the risk of obese adults being food insecure. The out-of-pocket costs or other medical costs associated with obesity-related comorbid conditions could increase the financial hardship in the home and lead to FI.12,13,46 Individuals living in food-insecure households often face competing priorities, e.g., having to choose between spending money on medications, transportation, or food. This could lead to a cycle by which obese adults develop comorbid conditions and then become food insecure, thus making it more difficult for them to make lifestyle modifications, lose weight, and improve their overall health.
Our results have both important clinical and public health significance. Obesity remains a national epidemic and improving weight status and nutrition is a top priority of HealthyPeople 2020.47, 48 Obesity treatment has changed with the development of new medications and surgical approaches, but lifestyle modification remains the mainstay of treatment.49, 50 Obese patients suffering from FI, though, may be less likely to comply with lifestyle changes due to limited resources, and FI may increase the risk of obese patients developing medical comorbidities. Obesity treatment guidelines have not included information about how to address FI as part of care though, and few clinicians systematically screen for FI.51,52
Also, increasing national organizations are recommending that health systems identify FI and other SDH in order to improve patient care and population health. A growing body of literature has developed strategies to address FI as a routine part of clinical care.6,7,8,53,54,55 Further research is needed to determine if addressing FI in clinical practices prevents the development of comorbid conditions, but clinicians and health systems could consider addressing FI to mitigate the broader social issues affecting patients. Prior studies have shown that addressing FI in clinical practices can improve the resources, such as access to local food pantries or nutritional assistance programs, patients receive.53,54,55 Clinicians could also advocate for policies that broaden the eligibility requirements and role of nutrition assistance programs, such as SNAP. SNAP has been shown to be effective in reducing household FI and expanding SNAP could further decrease FI and potentially comorbid conditions.56,57 Given the public health burden of obesity and FI, developing effective strategies for public health organizations and healthcare systems to address patient’s unmet food needs while promoting healthy lifestyle changes should continue to be a priority for future research.
This study has several limitations. First, we cannot determine causation with the cross-sectional design used in this study. Whether FI causes adults to develop obesity-related comorbidities or an increased number of comorbidities causes adults to be food insecure is unclear. Though our study was cross sectional, a strength of the design is the large, nationally representative sample to provide accurate results regarding FI. Second, several of the outcomes were measured using self-report. During the interview in NHANES, the participants are asked if a doctor told them they had a particular health condition. As food-insecure adults are less likely to seek preventative care,40,44 however, we would expect this to bias our results toward the null. In sensitivity analyses evaluating the association between FI and comorbidities that were directly measured in NHANES, we also found a small, but significant association between very low food security and the number of comorbidities. Third, we used propensity scores to improve covariate balance between food-secure and food-insecure participants. Propensity scores can only balance observed characteristics, and it is possible that imbalances remain due to unmeasured characteristics. Also, NHANES does not include data on other SDH, such as lack of transportation or housing instability, that often cluster with FI. So it is unclear if FI is a marker for some of these other SDH or on the causal pathway in the development of these comorbid conditions. Although some characteristics may have been unmeasured, there were many observed covariates, which we were able to include in our analysis and is consistent with previous studies.10,12,13, 28 Fourth, we did not include physical activity in our models. The physical activity assessment in NHANES underwent a change during the study period and could not be included. Physical inactivity has been considered a mediator between FI and chronic health conditions in prior conceptual models and studies;28,58 thus, we did not consider it to be a confounder in our results. Despite these limitations, our study provides robust results for assessing the association between FI and comorbid conditions.
CONCLUSION
Food insecurity and obesity remain major public health problems and lead to numerous negative health outcomes. In this nationally representative cohort, we found that obese adults who lived in food-insecure households were significantly more likely to have an increased number of comorbid medical conditions than obese, food-secure adults. Although further research is needed to determine causality and confirm our findings, clinicians should consider how FI might impact care when treating obese patients, particularly those with multiple comorbidities. Future studies should assess the effectiveness of methods for reducing FI and comorbid outcomes in obese individuals.
References
Solar O, Irwin A. A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2 (Policy and Practice). http://www.who.int/sdhconference/resources/ConceptualframeworkforactiononSDH_eng.pdf. Accessed 22 February 2019.
Mensah GA, Cooper RS, Siega-Riz AM, et al. Reducing Cardiovascular Disparities Through Community-Engaged Implementation Research: A National Heart, Lung, and Blood Institute Workshop Report. Circ Res 2018;122(2):213–230. https://doi.org/10.1161/CIRCRESAHA:117.312243
Marmot MG, Bosma H, Hemingway H, Brunner E, Stansfeld S. Contribution of job control and other risk factors to social variations in coronary heart disease incidence. Lancet 1997;350(9073):235–239.
Marmot M, Shipley M, Brunner E, Hemingway H. Relative contribution of early life and adult socioeconomic factors to adult morbidity in the Whitehall II study. J Epidemiol Community Health 2001;55(5):301–307.
Havranek EP, Mujahid MS, Barr DA, et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation.2015;132(9):873–898. https://doi.org/10.1161/CIR.00000000000000228.
Healthy People 2020: An Opportunity to Address Societal Determinants of Health in the United States. Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2020. U.S. Department of Health & Human Services. Available at: https://www.healthypeople.gov/2010/hp2020/advisory/societaldeterminantshealth.htm. Accessed 22 February 2019.
Billioux A, Verlander K, Anthony S, Alley D. Standardized Screening for Health-Related Social Needs in Clinical Settings: The accountable health communities screening tool. Discussion Paper, National Academy of Medicine, Washington D.C. 2017. https://nam.edu/wp-content/uploads/2017/05/Standardized-Screening-for-Health-Related-Social-Needs-in-Clinical-Settings.pdf. Accessed 22 February 2019.
Dzau VJ, McClellan MB, McGinnis JM, et al. Vital Directions for Health and Health Care: Priorities From a National Academy of Medicine Initiative. JAMA 2017;317(14):1461–1470. https://doi.org/10.1001/jama.2017.1964.
Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household Food Security in the United States in 2016, ERR-237. 2017. U.S. Department of Agriculture, Economic Research Service.
Berkowitz SA, Berkowitz TSZ, Meigs JB, Wexler DJ. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005-2012. PLoS One 2017;12(6):e0179172. https://doi.org/10.1371/journal.pone.0179172
Berkowitz SA, Seligman HK, Choudhry NK. Treat or eat: food insecurity, cost-related medication underuse, and unmet needs. Am J Med 2014;127(4):303–310 e303. https://doi.org/10.1016/j.amjmed.2014.01.002.
Seligman HK, Laraia BA, Kushel MB. Food insecurity is associated with chronic disease among low-income NHANES participants. J Nutr 2010;140(2):304–310. https://doi.org/10.3945/jn.109.112573.
Seligman HK, Bindman AB, Vittinghoff E, Kanaya AM, Kushel MB. Food insecurity is associated with diabetes mellitus: results from the National Health Examination and Nutrition Examination Survey (NHANES) 1999-2002. J Gen Intern Med 2007;22(7):1018–1023.
Berkowitz SA, Meigs JB, DeWalt D, et al. Material Need Insecurities, Control of Diabetes Mellitus, and Use of Health Care Resources: Results of the Measuring Economic Insecurity in Diabetes Study. JAMA Intern Med 2015; 175(2): 257–65. https://doi.org/10.1001/jamainternmed.2014.6888.
Shtasel-Gottlieb Z, Palakshappa D, Yang F, Goodman E. The relationship between developmental assets and food security in adolescents from a low-income community. J Adolesc Health 2015;56(2):215–222.
Gregory C, Coleman-Jensen A. Food Insecurity, Chronic Disease, and Health Among Working-Age Adults, ERR-235, U.S. Department of Agriculture, Economic Research Service, July 2017.
Vaccaro JA, Huffman FG. Sex and Race/Ethnic Disparities in Food Security and Chronic Diseases in U.S. Older Adults. Gerontol Geriatr Med 2017;3:2333721417718344. https://doi.org/10.1177/23333721417718344.
Franklin B, Jones A, Love D, Puckett S, Macklin J, White-Means S. Exploring mediators of food insecurity and obesity: a review of recent literature. J Community Health 2012;37(1):253–264. https://doi.org/10.1007/s10900-011-9420-4.
Bhattacharya J, Currie J, Haider S. Poverty, food insecurity, and nutritional outcomes in children and adults. J Health Econ 2004;23(4):839–862.
Casey PH, Simpson PM, Gossett JM, et al. The association of child and household food insecurity with childhood overweight status. Pediatrics 2006;118(5):e1406–1413.
Hunger and Obesity: Understanding a Food Insecurity Paradigm: Workshop Summary (2011). The National Academies Press. Available at: https://www.nap.edu/read/13102/chapter/1. Accessed on 22 February 2019.
Hanson KL, Connor LM. Food insecurity and dietary quality in US adults and children: a systematic review. Am J Clin Nutr 2014;100(2):684–692. https://doi.org/10.3945/ajcn.114.084525.
Drewnowski A, Specter SE. Poverty and obesity: the role of energy density and energy costs. Am J Clin Nutr 2004;79(1):6–16.
Gunter KB, Jackson J, Tomayko EJ, John DH. Food insecurity and physical activity insecurity among rural Oregon families. Prev Med Rep 2017;8:38–41. https://doi.org/10.1016/j.pmedr.2017.07.006.
To QG, Frongillo EA, Gallegos D, Moore JB. Household food insecurity is associated with less physical activity among children and adults in the U.S. population. J Nutr 2014;144(11):1797–1802. https://doi.org/10.3945/jn.114.198184.
About the National Health and Nutrition Examination Survey. National Center of Health Statistics. Available at https://http://www.cdc.gov/nchs/nhanes/about_nhanes.htm. Accessed on 22 February 2019.
Household Food Security in the United States in 1995: Summary Report of the Food Security Measurement Project. U.S. Department of Agriculture, Food and Consumer Service. September 1997. Available at: https://www.fns.usda.gov/household-food-security-united-states-1995-summary-report-food-security-measurement-project. Accessed on 22 February 2019.
Berkowitz SA, Baggett TP, Wexler DJ, Huskey KW, Wee CC. Food insecurity and metabolic control among U.S. adults with diabetes. Diabetes Care 2013;36(10):3093–3099. https://doi.org/10.2337/dc13-0570.
Huntley AL, Johnson R, Purdy S, Valderas JM, Salisbury C. Measures of multimorbidity and morbidity burden for use in primary care and community settings: a systematic review and guide. Ann Fam Med 2012;10(2):134–141. https://doi.org/10.1370/afm.1363.
de Groot V, Beckerman H, Lankhorst GJ, Bouter LM. How to measure comorbidity. a critical review of available methods. J Clin Epidemiol 2003;56(3):221–229.
Obesity and Cancer. National Cancer Institute. Available at: https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/obesity-fact-sheet. Accessed 22 February 2019.
Fryar CD, Carroll MD, Ogden CL. Prevalence of overweight, obesity and extreme obesity among adults: United States, 1960-1962 through 2011-2012. National Center for Health Statistics. Available at: https://www.cdc.gov/nchs/data/hestat/obesity_adult_11_12/obesity_adult_11_12.htm. Accessed 22 February 2019.
The R Project for Statistical Computing. Available at: http://www.R-project.org/. Accessed 22 February 2019.
Rossen LM, Kobernik EK. Food insecurity and dietary intake among US youth, 2007-2010. Pediatr Obes 2016;11(3):187–193. https://doi.org/10.1111/ijpo.12044.
Ladapo JA, Richards AK, DeWitt CM, et al. Disparities in the Quality of Cardiovascular Care Between HIV-Infected Versus HIV-Uninfected Adults in the United States: A Cross-Sectional Study. J Am Heart Assoc 2017;6(11). https://doi.org/10.1161/JAHA.117.007107.
Dugoff EH, Schuler M, Stuart EA. Generalizing observational study results: applying propensity score methods to complex surveys. Health Serv Res 2014;49(1):284–303. https://doi.org/10.1111/1475-6773.
Liaw A, Wiener M. Classification and regression by randomForest. R news 2.3. 2002:18–22.
Lee BK, Lessler J, Stuart EA. Improving propensity score weighting using machine learning. Stat Med 2010;29(3):337–346. https://doi.org/10.1002/sim.3782.
Weiser SD, Palar K, Hatcher A, Young S, Frongillo E, Laraia B. 2015. Food Insecurity and Health: A Conceptual Framework. In L. Ivers (ed.), Food Insecurity and Public Health (pp. 23–50). CRC Press.
Kushel MB, Gupta R, Gee L, Haas JS. Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med 2006;21(1):71–77.
Rosmond R, Dallman MF, Bjorntorp P. Stress-related cortisol secretion in men: relationships with abdominal obesity and endocrine, metabolic and hemodynamic abnormalities. J Clin Endocrinol Metab 1998;83(6):1853–1859.
Dixon LB, Winkleby MA, Radimer KL. Dietary intakes and serum nutrients differ between adults from food-insufficient and food-sufficient families: Third National Health and Nutrition Examination Survey, 1988-1994. J Nutr 2001;131(4):1232–1246.
Whitaker RC, Phillips SM, Orzol SM. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics. 2006;118(3):e859–868.
Charkhchi P, Fazeli Dehkordy S, Carlos RC. Housing and Food Insecurity, Care Access, and Health Status Among the Chronically Ill: An Analysis of the Behavioral Risk Factor Surveillance System. J Gen Intern Med 2018;33(5): 644–650. https://doi.org/10.1007/s11606-017-4255-z.
Laraia BA. Food insecurity and chronic disease. Adv Nutr 2013;4(2):203–212. https://doi.org/10.3945/an.112.003277.
Jih J, Stijacic-Cenzer I, Seligman HK, Boscardin WJ, Nguyen TT, Ritchie CS. Chronic disease burden predicts food insecurity among older adults. Public Health Nutr1 2018:1–6. https://doi.org/10.1017/S1368980017004062.
Overweight & Obesity. Centers for Disease Control and Prevention. Available at: https://http://www.cdc.gov/obesity/data/prevalence-maps.html. Accessed 22 February 2019.
Nutrition and Weight Status. Office of Disease Prevention and Health Promotion. Avilable at: https://http://www.healthypeople.gov/2020/topics-objectives/topic/nutrition-and-weight-status. Accessed 22 February 2019.
Lewis KH, Edwards-Hampton SA, Ard JD. Disparities in Treatment Uptake and Outcomes of Patients with Obesity in the USA. Curr Obes Rep 2016;5(2):282–290. https://doi.org/10.1007/s13679-016-0211-1.
Eckel RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2960–2984. https://doi.org/10.1016/j.jacc.2013.11.003.
Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol2014;63(25 Pt B):2985–3023. https://doi.org/10.1016/j.jacc.2013.11.004.
Hoisington AT, Braverman MT, Hargunani DE, Adams EJ, Alto CL. Health care providers’ attention to food insecurity in households with children. Prev Med 2012;55(3):219–222. https://doi.org/10.1016/j.ypmed.2012.06.007.
Berkowitz SA, Hulberg AC, Standish S, Reznor G, Atlas SJ. Addressing Unmet Basic Resource Needs as Part of Chronic Cardiometabolic Disease Management. JAMA Intern Med 2017;177(2):244–252. https://doi.org/10.1001/jamainternmed.2016.7691.
Garg A, Toy S, Tripodis Y, Silverstein M, Freeman E. Addressing social determinants of health at well child care visits: a cluster RCT. Pediatrics. 2015;135(2):e296–304.
Gottlieb LM, Hessler D, Long D, et al. Effects of Social Needs Screening and In-Person Service Navigation on Child Health: A Randomized Clinical Trial. JAMA Pediatr 2016:e162521.
Swann CA. Household history, SNAP participation, and food insecurity. Food Policy 2017;73:1–9.
Gunderson C, Kreider B, Pepper JV. Partial Identification Methods for Evaluating Food Assistance Programs: A Case Study of the Causal Impact of SNAP on Food Insecurity. Am J Agric Econ 2017;99(4):875–893.
Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. N Engl J Med 2010;363(1):6–9. https://doi.org/10.1056/NEJMp1000072.
Acknowledgments
Portions of this study were presented at the Society for General Internal Medicine in April 2018 in Denver, CO.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 39 kb)
Rights and permissions
About this article

Cite this article
Palakshappa, D., Speiser, J.L., Rosenthal, G.E. et al. Food Insecurity Is Associated with an Increased Prevalence of Comorbid Medical Conditions in Obese Adults: NHANES 2007–2014. J GEN INTERN MED 34, 1486–1493 (2019). https://doi.org/10.1007/s11606-019-05081-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-019-05081-9