
Abstract
BACKGROUND
Failure to reconcile medications across transitions in care is an important source of harm to patients. Little is known about medication discrepancies upon admission to skilled nursing facilities (SNFs).
OBJECTIVE
To describe the prevalence of, type of medications involved in, and sources of medication discrepancies upon admission to the SNF setting.
DESIGN
Cross-sectional study.
PARTICIPANTS
Patients admitted to SNF for subacute care.
MEASUREMENTS
Number of medication discrepancies, defined as unexplained differences among documented medication regimens, including the hospital discharge summary, patient care referral form and SNF admission orders.
RESULTS
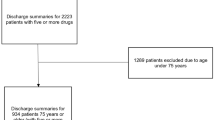
Of 2,319 medications reviewed on admission, 495 (21.3%) had a medication discrepancy. At least one medication discrepancy was identified in 142 of 199 (71.4%) SNF admissions. The discharge summary and the patient care referral form did not match in 104 of 199 (52.3%) SNF admissions. Disagreement between the discharge summary and the patient care referral form accounted for 62.0% (n = 307) of all medication discrepancies. Cardiovascular agents, opioid analgesics, neuropsychiatric agents, hypoglycemics, antibiotics, and anticoagulants accounted for over 50% of all discrepant medications.
CONCLUSIONS
Medication discrepancies occurred in almost three out of four SNF admissions and accounted for one in five medications prescribed on admission. The discharge summary and the patient care referral forms from the discharging institution are often in disagreement. Our study findings underscore the importance of current efforts to improve the quality of inter-institutional communication.

Similar content being viewed by others

References
Coleman EA, Smith JD, Raha D, et al. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165:1842–7.
The Joint Commission. 2008 National Patient Safety Goals - Long-term Care Program [On-line] http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ 08_ltc_npsgs.htm. Accessed February 13, 2009.
Santell JP. Reconciliation failures lead to medication errors. J Qual Patient Saf. 2006;32:225–9.
Tam VC, Knowles SR, Cornish PL, et al. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005;173:510–5.
Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165:424–9.
Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166:565–71.
Wong JD, Bajcar JM, Wong GG, et al. Medication reconciliation at hospital discharge: evaluating discrepancies. Ann Pharmacother. 2008;42:1373–9.
Vira T, Colquhoun M, Etchells E. Reconcilable differences: correcting medication errors at hospital admission and discharge. Qual Saf Health Care. 2006;15:122–6.
Wong JD, Bajcar JM, Wong GG, et al. Medication reconciliation at hospital discharge: evaluating discrepancies. Ann Pharmacother. 2008;42:1373–9.
Liu K, Garrett B, Wissoker D, et al. Options for improving medicare payment for skilled nursing facilities: Centers for Medicare and Medicaid Services (CMS); 2007. Available at: http://www.urban.org/url.cfm?ID=411526. Accessed February 13, 2009.
Yip JY, Wilber KH, Myrtle RC. The impact of the 1997 Balanced Budget Amendment's prospective payment system on patient case mix and rehabilitation utilization in skilled nursing. Gerontologist. 2002;42:653–60.
Michaud Y, ed. A systems approach to quality improvement in long-term care: safe medication practices workbook. Massachusetts Coalition to Prevent Medical Errors. 2007. Available at: http://www.masspro.org/NH/docs/tools/SafeMedPrac06_8-07Upd.pdf. Accessed February 13, 2009.
Wilson S, Ruscoe W, Chapman M, Miller R. General practitioner-hospital communications: a review of discharge summaries. J Qual Clin Pract. 2001;21:104–8.
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–41.
Lisby M, Nielsen LP, Mainz J. Errors in the medication process: frequency, type, and potential clinical consequences. Int J Qual Health Care. 2005; 17: 15–22.
Nickerson A, MacKinnon NJ, Roberts N, Saulnier L. Drug-therapy problems, inconsistencies and omissions identified during a medication reconciliation and seamless care service. Healthc Q. 2005;8:65–72.
Varkey P, Cunningham J, O'Meara J, Bonacci R, Desai N, Sheeler R. Multidisciplinary approach to inpatient medication reconciliation in an academic setting. Am J Health Syst Pharm. 2007;64:850–4.
Soumerai SB, Avorn J, Ross-Degnan D, et al. Payment restriction for prescription drugs under Medicaid. N Engl J Med. 1987;317:1072–7.
Soumerai SB, Ross-Degnan D, Avorn J, et al. Effects of Medicaid drug-payment limits on admission to hospitals and nursing homes. N Engl J Med. 1991;325:1072–7.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161–7.
Boockvar K, Fishman E, Kyriacou CK, Monias A, Gavi S, Cortes T. Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med. 2004;164:545–50.
Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after discharge from hospital. CMAJ. 2004;170:345–9.
Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients–development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354–60.
Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization. Ann Intern Med. 2009;150:178–87.
Medicare Payment Advisory Commission. Report to the Congress: Promoting greater efficiency in Medicare. 2007. Available at: http://www.medpac.gov/documents/ Jun07_EntireReport.pdf. Accessed February 13, 2009.
Acknowledgements
We gratefully acknowledge Jerry Gurwitz, MD, for his support of this project, the work of the research team advance practice nurses Francisca Adams, Suzanne Sullivan, and Anne Crowell, research assistant Diane Quinn, and Jennifer Donovan, PharmD, Abir Kanaan, Pharm D, and Jane L. Givens, MD, MSCE, for their assistance with this manuscript.
Funding/support
Dr. Tjia was supported by a Mentored Clinical Scientist Career Development Award from the National Institute on Aging (K08 AG021527). This study was supported by a grant from the Rosalie Wolf Interdisciplinary Geriatric Health Care Research Center at the University of Massachusetts Medical School and the University of Massachusetts Boston funded by the John A. Hartford Foundation and the RAND Corporation.
Financial Disclosures
Dr. Briesacher has received unrestricted research grants from and served as a consultant for Novartis Pharmaceutical Corporation within the past 3 years.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tjia, J., Bonner, A., Briesacher, B.A. et al. Medication Discrepancies upon Hospital to Skilled Nursing Facility Transitions. J GEN INTERN MED 24, 630–635 (2009). https://doi.org/10.1007/s11606-009-0948-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-009-0948-2