
Abstract
Background
As an increasing number of patients with chronic conditions of childhood survive to adulthood, experts recommend that young adults with chronic conditions transfer from child-focused to adult-focused primary care. Little, however, is known about how comfortable physicians are caring for this population.
Objectives
To assess the comfort of general internists and general pediatricians in treating young adult patients with chronic illnesses originating in childhood as well as the factors associated with comfort.
Participants
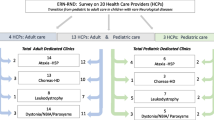
In a random sample, 1288 of 2434 eligible US general internists and pediatricians completed a mailed survey (response rate = 53%).
Methods
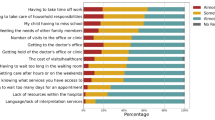
We measured respondents’ comfort level in providing primary care for a patient with sickle cell disease (SCD) or cystic fibrosis (CF). We also measured levels of disease familiarity, training and subspecialty support, as well as individual physician characteristics.
Results
Fifteen percent of general internists reported being comfortable as the primary care provider for adults with CF and 32% reported being comfortable providing primary care for adults with SCD, compared with 38% of pediatricians for CF (p < .001) and 35% for SCD (p > 0.05). Less than half of general internists felt that their specialty should take primary care responsibility for adult patients with CF and SCD.
Conclusions
A majority of general internists and pediatricians are not comfortable providing primary care for young adults with chronic illnesses of childhood origin, such as CF and SCD. Efforts to increase treatment comfort among providers may help with the transition to adult-focused care for the growing numbers of young adults with complex chronic conditions.
Similar content being viewed by others

Abbreviations
- CF:
-
cystic fibrosis
- PCP:
-
primary care physician
- SCD:
-
sickle cell disease
References
Elborn JS, Shale DJ, Britton JR. Cystic fibrosis: current survival and population estimates to the year 2000. Thorax. 1991;46(12):881–5.
Reid GJ, Webb GD, Barzel M, McCrindle BW, Irvine MJ, Siu SC. Estimates of life expectancy by adolescents and young adults with congenital heart disease. J Am Coll Cardiol. 2006;482:349–55.
Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease. Life expectancy and risk factors for early death. N Engl J Med. 1994;330(23):1639–44.
Warnes CA, Liberthson R, Danielson GK, et al. Task force 1: the changing profile of congenital heart disease in adult life. J Am Coll Cardiol. 2001;375:1170–5.
Lakdawalla DN, Bhattacharya J, Goldman DP. Are the young becoming more disabled? Health Aff (Millwood). 2004;231:168–76.
Newacheck PW, Strickland B, Shonkoff JP, et al. An epidemiologic profile of children with special health care needs. Pediatrics. 1998;102(1 Pt 1):117–23.
van der Lee J, Mokkink L, Grootenhuis M, Heymans H, Offringa M. Definitions and measurement of chronic health conditions in childhood: a systematic review. JAMA. 2007;297(24):2741–51. 1999 Oct.
Blum RW, Garell D, Hodgman CH, et al. Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine. J Adolesc Health. 1993;147:570–6.
American Academy of Pediatrics, American Academy of Family Physicians, American College of Physicians-American Society of Internal Medicine. A consensus statement on health care transitions for young adults with special health care needs. Pediatrics. 2002;110(6 Pt 2):1304–6.
Reschovsky J, Reed M, Blumenthal D, Landon B. Physicians’ assessments of their ability to provide high-quality care in a changing health care system. Med Care. 2001;39(3):254–69.
Foster GD, Wadden TA, Makris AP, et al. Primary care physicians’ attitudes about obesity and its treatment. Obes Res. 2003;11(10):1168–77.
Blum R. Physicians’ assessment of deficiencies and desire for training in adolescent care. J Med Educ. 1987;62(5):401–7.
Zimmerman DL, Selick A, Singh R, Mendelssohn DC. Attitudes of Canadian nephrologists, family physicians and patients with kidney failure toward primary care delivery for chronic dialysis patients. Nephrol Dial Transplant. 2003;18(2):305–9.
Schidlow DV, Fiel SB. Life beyond pediatrics. Transition of chronically ill adolescents from pediatric to adult health care systems. Med Clin North Am. 1990;74(5):1113–20.
Stille CJ, Jerant A, Bell D, Meltzer D, Elmore JG. Coordinating care across diseases, settings, and clinicians: a key role for the generalist in practice. Ann Intern Med. 2005;142(8):700–8.
Cabana MD, Rand CS, Becher OJ, Rubin HR. Reasons for pediatrician nonadherence to asthma guidelines. Arch Pediatr Adolesc Med. 2001;155(9):1057–62.
Miller AR, Johnston C, Klassen AF, Fine S, Papsdorf M. Family physicians’ involvement and self-reported comfort and skill in care of children with behavioral and emotional problems: a population-based survey. BMC Fam Pract. 2005;6:(1)12.
Forrest CB, Nutting PA, von Schrader S, Rohde C, Starfield B. Primary care physician specialty referral decision making: patient, physician, and health care system determinants. Med Decis Making. 2006;26(1):76–85.
Williams JW, Rost K, Dietrich AJ, Ciotti MC, Zyzanski SJ, Cornell J. Primary care physicians’ approach to depressive disorders. Effects of physician specialty and practice structure. Arch Fam Med. 1999;8(1):58–67.
Scal P. Transition for youth with chronic conditions: primary care physicians’ approaches. Pediatrics. 2002;110(6 Pt 2):1315–21.
Geenen SJ, Powers LE, Sells W. Understanding the role of health care providers during the transition of adolescents with disabilities and special health care needs. J Adolesc Health. 2003;32(3):225–33.
Donaldson MS, Yordy KD, Lohr KN, Vanselow NA. Primary Care: America’s Health in a New Era. Washington, D.C.: National Academy Press; 1996.
Frankel L. The report of the CASRO task force on response rates. In: Wiseman F, eds. The Report of the CASRO Task Force on Response Rates. Cambridge, MA: Marketing Science Institute; 1983.
Moore JL, McAuley JW, Mott D, Reeves AL, Bussa B. Referral characteristics of primary care physicians for seizure patients. Epilepsia. 2000;41(6):744–8.
Shah P, Norlin C, Logsdon V, Samson-Fang L. Gynecological care for adolescents with disability: physician comfort, perceived barriers, and potential solutions. J Pediatr Adolesc Gynecol. 2005;18(2):101–4.
Cummings SM, Savitz LA, Konrad TR. Reported response rates to mailed physician questionnaires. Health Serv Res. 2001;35(6):1347–55.
Carroll G, Massarelli E, Opzoomer A, et al. Adolescents with chronic disease. Are they receiving comprehensive health care? J Adolesc Health Care. 1983;4(4):261–5.
Harrold LR, Field TS, Gurwitz JH. Knowledge, patterns of care, and outcomes of care for generalists and specialists. J Gen Intern Med. 1999;14(8):499–511.
Donohoe MT. Comparing generalist and specialty care: discrepancies, deficiencies, and excesses. Arch Intern Med. 1998;158(15):1596–608.
Acknowledgements
We wish to thank Dylan Smith and Norbert Schwarz for psychometric input on the survey; Samya Nasr and Andrew Campbell for disease specific input to the clinical vignette; Paula Lantz for her generous insight regarding the survey items; Camilla Payne for editing. We also received biostatistical assistance from the BREAD of the UCSF CTSI (Grant #UL1 RR024131).
Conflicts of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was funded by the Robert Wood Johnson Clinical Scholars Program and the UCSF Division of Pediatrics. Dr. Heisler is a VA Health Services Research and Development Career Development Awardee.
Appendix
Appendix
Physicians were randomized to receive a CF or SCD clinical vignette to anchor their answers to the question who would be the best primary care provider to a patient.
Cystic fibrosis clinical vignette:
An 18-year-old woman with cystic fibrosis comes to your office to establish care. Her medical history is significant for multiple pulmonary infections and pancreatic insufficiency. Today she would like to discuss with you her chronic cough, increased sputum production, chronic back pain, dysmenorrhea and cystic fibrosis management.
Sickle cell disease clinical vignette
An 18-year-old woman with sickle cell disease comes to your office to establish care. Her medical history is significant for multiple pain crises, complicated by acute chest syndrome and an intracranial hemorrhage in the past. Today she would like to discuss with you her chronic back pain, dysmenorrhea and sickle cell management.
We then asked the following question:
Who do you feel would be best to provide for the primary care needs for young adults (17–25 years old) with sickle cell disease/cystic fibrosis?
Response choices included pediatric generalist, pediatric pulmonologist or hematologist, adult generalist, adult pulmonologist or hematologist or other depending on vignette.
Rights and permissions
About this article
Cite this article
Okumura, M.J., Heisler, M., Davis, M.M. et al. Comfort of General Internists and General Pediatricians in Providing Care for Young Adults with Chronic Illnesses of Childhood. J GEN INTERN MED 23, 1621–1627 (2008). https://doi.org/10.1007/s11606-008-0716-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-008-0716-8