
Abstract
Introduction
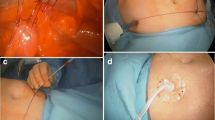
Adequate perioperative nutrition is critical for the success of surgical outcomes. Jejunostomy feeding tube placement may ensure enteral feeding access; however, these types of tubes have had variable reported rates of dysfunction/morbidity. The aim of our study was to report our experience with jejunostomy feeding tube placement and the long-term outcomes following complex foregut surgery.
Methods
We performed a review of all of our jejunostomy feeding tube placement patients from 1/1/2010 until 7/1/2018. The indication for surgery and primary operation were recorded. All adverse events related to the jejunostomy were recorded during the entire duration of tube access. Social “hassle-factor” issues were also reported, including the number of “jejunostomy-related” phone calls, reinsertion and related placement studies, and readmissions pertaining to jejunostomy-associated complications.
Results
During the study period, 542 primary procedures were performed with secondary jejunostomy placement. Jejunostomy-related adverse events occurred in 22.0% of patients (n = 119/542); 12.0% (n = 65/542) were dislodged tubes, 6.0% (n = 30/542) clogged tubes; 5% (n = 25/542) leaking tubes, and 2.8% (n = 15/542) site infections. Tube dysfunctions initiated 244 reinsertion/placement studies in 107 patients, 20 jejunostomy tube-related readmissions, and 78 phone calls to providers for tube dysfunction. Adverse event rates differed significantly between groups (p < 0.001), with esophagogastric resection adverse event rates of 42.3% versus 19.2% for pancreatic ablations.
Discussion
Jejunostomy feeding tubes resulted in adverse events in less than a third of patients. Patient-related hassle must be communicated preoperatively in order to prevent jejunostomy tube-related morbidity. Optimal early and late jejunostomy feeding optimization varies based on preoperative patient comorbidities, type of operation, and the need for adjuvant oncology therapy.
Similar content being viewed by others


References
Mason MC, Garcia JM, Sansgiry S, Walder A, Berger DH, Anaya DA. Preoperative cancer cachexia and short-term outcomes following surgery. J Surg Res 2016;205(2):398–406.
Andersen HK, Lewis SJ, Thomas S. Early enteral nutrition within 24 h of colorectal surgery versus later commencement of feeding for postoperative complications. Cochrane Database Syst Rev 2006(4):CD004080.
Wheble GA, Knight WR, Khan OA. Enteral vs total parenteral nutrition following major upper gastrointestinal surgery. Int J Surg 2012;10(4):194–7.
DiSario JA. Endoscopic approaches to enteral nutritional support. Best Pract Res Clin Gastroenterol 2006;20(3):605–30.
Dann GC, Squires MH, 3rd, Postlewait LM, Kooby DA, Poultsides GA, Weber SM, et al. An assessment of feeding jejunostomy tube placement at the time of resection for gastric adenocarcinoma: A seven-institution analysis of 837 patients from the U.S. gastric cancer collaborative. J Surg Oncol 2015;112(2):195–202.
Alvarez-Sarrado E, Mingol Navarro F, JR Rosellón, Ballester Pla N, Vaqué Urbaneja FJ, Muniesa Gallardo C, et al. Feeding Jejunostomy after esophagectomy cannot be routinely recommended. Analysis of nutritional benefits and catheter-related complications. Am J Surg 2019;217(1):114–20.
Shumer EMRCG. Minimally invasive feeding tube and esophageal stent placement. Minimally invasive foregut surgery for malignancy: Principles and practice 2015;1:183–8.
Aoyagi T, Terracina KP, Raza A, Matsubara H, Takabe K. Cancer cachexia, mechanism and treatment. World J Gastrointest Oncol 2015;7(4):17–29.
Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr 2017;36(1):11–48.
Gyan E, Raynard B, Durand JP, Lacau Saint Guily J, Gouy S, Movschin ML, et al.. Malnutrition in Patients With Cancer: Comparison of Perceptions by Patients, Relatives, and Physicians-Results of the NutriCancer2012 Study. JPEN J Parenter Enteral Nutr 2018;42(1):255–60.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
O’Neill, C.H., Moore, J., Philips, P. et al. Complications of Jejunostomy Feeding Tubes: A Single Center Experience of 546 Cases. J Gastrointest Surg 24, 959–963 (2020). https://doi.org/10.1007/s11605-020-04529-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-020-04529-2