
Abstract
Background and Aim
Enteral stents (ES) have emerged as first-line therapy for the treatment of malignant gastric outlet obstruction (GOO). Stent occlusion arising from tissue ingrowth may require endoscopic or surgical reintervention. The objective of this study was to compare rates of reintervention following palliative ES for patients with GOO due to pancreatic adenocarcinoma (PDAC) versus other malignant etiologies.
Methods
Patients who had undergone ES for palliation of malignant GOO between 2009 and 2018 were retrospectively identified and demographic, clinical, and procedural data were collected. Primary outcome was procedural reintervention for recurrent symptomatic GOO following ES placement.
Results
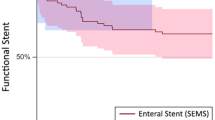
Forty-three patients were included in the study cohort. 62.8% (27/43) of patients had PDAC while 37.2% (16/43) of patients had other malignant etiologies. 11.6% (5/43) of patients were alive at follow-up. Thirty-day and 90-day mortality rates were 22.8% and 70.7% for PDAC and 25% and 56.3% for other malignant etiologies, respectively. Seven patients required reintervention for symptomatic GOO: 14.3% (1/7) had PDAC and 85.7% (6/7) had GOO due to other malignancy (P < .01). Ninety-six percent (26/27) of patients with PDAC required no further intervention for GOO prior to death or end of follow-up. On multivariate analysis, patients with PDAC were significantly less likely to require reintervention than patients with other malignant etiologies (OR 0.064, 95% CI 0.01–0.60).
Conclusion
ES offer durable symptom palliation without requirement for reintervention for the overwhelming majority of patients with malignant GOO due to PDAC. Reintervention rates are higher following ES placement for GOO due to other malignant etiologies and future study may be needed to define the optimal palliative intervention for this group of patients.



Similar content being viewed by others


References
Uemura S, Iwashita T, Iwata K, et al. Endoscopic duodenal stent versus surgical gastrojejunostomy for gastric outlet obstruction in patients with advanced pancreatic cancer. Pancreatology. 2018.
Goldberg EM. Palliative treatment of gastric outlet obstruction in terminal patients: SEMS. Stent every malignant stricture! Gastrointest Endosc. 2014;79(1):76–78.
Chen YI, Khashab MA. Endoscopic approach to gastrointestinal bypass in malignant gastric outlet obstruction. Curr Opin Gastroenterol. 2016.
Espinel J, Sanz O, Vivas S, et al. Malignant gastrointestinal obstruction: endoscopic stenting versus surgical palliation. Surg Endosc. 2006;20(7):1083–1087.
Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. Am J Gastroenterol. 2002;97(1):72–78.
Maetani I, Tada T, Ukita T, Inoue H, Sakai Y, Nagao J. Comparison of duodenal stent placement with surgical gastrojejunostomy for palliation in patients with duodenal obstructions caused by pancreaticobiliary malignancies. Endoscopy. 2004;36(1):73–78.
Dormann A, Meisner S, Verin N, Wenk Lang A. Self-expanding metal stents for gastroduodenal malignancies: systematic review of their clinical effectiveness. Endoscopy. 2004;36(6):543–550.
Khashab M, Alawad AS, Shin EJ, et al. Enteral stenting versus gastrojejunostomy for palliation of malignant gastric outlet obstruction. Surg Endosc. 2013;27(6):2068–2075.
Ly J, O’Grady G, Mittal A, Plank L, Windsor JA. A systematic review of methods to palliate malignant gastric outlet obstruction. Surg Endosc. 2010;24(2):290–297.
Piesman M, Kozarek RA, Brandabur JJ, et al. Improved oral intake after palliative duodenal stenting for malignant obstruction: a prospective multicenter clinical trial. Am J Gastroenterol. 2009;104(10):2404–2411.
Siddiqui A, Spechler SJ, Huerta S. Surgical bypass versus endoscopic stenting for malignant gastroduodenal obstruction: a decision analysis. Dig Dis Sci. 2007;52(1):276–281.
Roy A, Kim M, Christein J, Varadarajulu S. Stenting versus gastrojejunostomy for management of malignant gastric outlet obstruction: comparison of clinical outcomes and costs. Surg Endosc. 2012;26(11):3114–3119.
Evans JA, Chandrasekhara V, Chathadi KV, et al. The role of endoscopy in the management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015;82(1):1–8.
Tringali A, Didden P, Repici A, et al. Endoscopic treatment of malignant gastric and duodenal strictures: a prospective, multicenter study. Gastrointest Endosc. 2014;79(1):66–75.
Oh D, Lee SS, Song TJ, et al. Efficacy and safety of a partially covered duodenal stent for malignant gastroduodenal obstruction: a pilot study. Gastrointest Endosc. 2015;82(1):32–36.e31.
Oh SY, Edwards A, Mandelson M, et al. Survival and clinical outcome after endoscopic duodenal stent placement for malignant gastric outlet obstruction: comparison of pancreatic cancer and nonpancreatic cancer. Gastrointest Endosc. 2015;82(3):460–468.e462.
Jeurnink SM, Steyerberg EW, van Hooft JE, et al. Surgical gastrojejunostomy or endoscopic stent placement for the palliation of malignant gastric outlet obstruction (SUSTENT study): a multicenter randomized trial. Gastrointest Endosc. 2010;71(3):490–499.
Itoi T, Ishii K, Ikeuchi N, et al. Prospective evaluation of endoscopic ultrasonography-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) for malignant gastric outlet obstruction. Gut. 2016;65(2):193–195.
Chen YI, Kunda R, Storm AC, et al. EUS-guided gastroenterostomy: a multicenter study comparing the direct and balloon-assisted techniques. Gastrointest Endosc. 2018;87(5):1215–1221.
Itoi T, Baron TH, Khashab MA, et al. Technical review of endoscopic ultrasonography-guided gastroenterostomy in 2017. Dig Endosc. 2017;29(4):495–502.
Khashab MA, Bukhari M, Baron TH, et al. International multicenter comparative trial of endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for the treatment of malignant gastric outlet obstruction. Endosc Int Open. 2017;5(4):E275-E281.
Chen YI, Itoi T, Baron TH, et al. EUS-guided gastroenterostomy is comparable to enteral stenting with fewer re-interventions in malignant gastric outlet obstruction. Surg Endosc. 2017;31(7):2946–2952.
Ratone JP, Caillol F, Zemmour C, et al. Outcomes of duodenal stenting: Experience in a French tertiary center with 220 cases. Dig Liver Dis. 2019.
Sterpetti AV, Fiori E, Sapienza P, Lamazza A. Complications After Endoscopic Stenting for Malignant Gastric Outlet Obstruction: A Cohort Study. Surg Laparosc Endosc Percutan Tech. 2019;29(3):169–172.
Author information
Authors and Affiliations
Contributions
Jordan Orr and Patrick Yachimski contributed in study concept and design, analysis and interpretation of data, and drafting of the manuscript. James C. Slaughter contributed in analysis and interpretation of the data. Robert Lockwood, Anthony Gamboa, Keith L. Obstein, and Patrick Yachimski contributed in critical revision of the article for important intellectual content. All authors approve the final draft submitted.
Corresponding author
Ethics declarations
Institutional review board approval was obtained to conduct this single-center, retrospective study.
Conflict of Interest
Patrick Yachimski is a consultant for Boston Scientific. Jordan Orr, Robert Lockwood, Anthony Gamboa, James C. Slaughter, and Keith L. Obstein have no conflicts of interest to disclose. We have no sources of funding or other types of assistance to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Orr, J., Lockwood, R., Gamboa, A. et al. Enteral Stents for Malignant Gastric Outlet Obstruction: Low Reintervention Rates for Obstruction due to Pancreatic Adenocarcinoma Versus Other Etiologies. J Gastrointest Surg 25, 720–727 (2021). https://doi.org/10.1007/s11605-019-04512-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-019-04512-6