
Abstract
Background and Purpose
Publications document the risk of developing esophageal stricture as a sequential complication of esophageal injury grades 2b and 3a. Although there are studies describing the risk factors of post-corrosive stricture, there is limited literature on these factors. The aim of this study was to evaluate the different factors with post-corrosive esophageal stricture and non-stricture groups in endoscopic grades 2b and 3a of corrosive esophageal injuries.
Methods
Data were retrospectively analyzed in the patients with esophageal injury grades 2b and 3a between January 2011 and December 2017.
Results
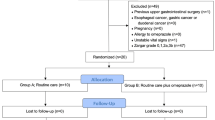
One hundred ninety-six corrosive ingestion patients were admitted with 32 patients (15.8%) in grade 2b and 12 patients (6.1%) in grade 3a and stricture was developed in 19 patients (61.3%) with grade 2b and in 10 patients (83.3%) with grade 3a. The patients’ height of the non-stricture group was greater than that of stricture groups (2b stricture group, 1.58 ± 0.08 m; 2b non-stricture group, 1.66 ± 0.07 m; p < 0.004; 3a stricture group, 1.52 ± 0.09 m; 3a non-stricture group, 1.71 ± 0.02 m; p < 0.001). Omeprazole was more commonly used in the non-stricture than stricture group (26.3% in the 2b stricture group, 69.2% in the 2b non-stricture group, p = 0.017; 50% in the 3a stricture group, 100% in the 3a non-stricture group, 1.71 ± 0.02 m, p = 0.015).
Conclusions
The height of patients may help to predict the risks and the prescription of omeprazole may help to minimize the risks of 2b and 3a post-corrosive esophageal stricture.
Similar content being viewed by others


References
Havanond C. Clinical features of corrosive ingestion. J Med Assoc Thai. 2003;86(10):918–24.
Awsakulsutthi S, Havanond C. A retrospective study of anastomotic leakage between patients with and without vascular enhancement of esophageal reconstructions with colon interposition: Thammasat University Hospital experience. Asian J Surg. 2015;38(3):145–9.
Havanond C, Havanond P. Initial signs and symptoms as prognostic indicators of severe gastrointestinal tract injury due to corrosive ingestion. J Emerg Med. 2007;33(4):349–53.
Havanond C. Is there a difference between the management of grade 2b and 3 corrosive gastric injuries? J Med Assoc Thai. 2002;85(3):340–4.
Contini S, Scarpignato C. Caustic injury of the upper gastrointestinal tract: a comprehensive review. World J Gastroenterol. 2013;19(25):3918–30.
Are’valo-Silva C, Eliashar R, Wohlgelernter J, Elidan J, Gross M. Ingestion of caustic substances: a 15-year experience. Laryngoscope. 2006;116(8):1422–6.
Pace F, Antinori S, Repici A. What is new in esophageal injury (infection, drug-induced, caustic, stricture, perforation)? Curr Opin Gastroenterol. 2009;25(4):372–9.
Hugh TB, Kelly MD. Corrosive ingestion and the surgeon. J Am Coll Surg. 1999;189(5):508–22.
Goldman LP, Weigert JM. Corrosive substance ingestion: a review. Am J Gastroenterol 1984;79:85–90.
Zargar SA, Kochhar R, Nagi B, Mehta S, Mehta SK. Ingestion of corrosive acids. Spectrum of injury to upper gastrointestinal tract and natural history. Gastroenterology. 1989;97(3):702–7.
Zargar SA, Kochhar R, Nagi B, Mehta S, Mehta SK. Ingestion of strong corrosive alkalis: spectrum of injury to upper gastrointestinal tract and natural history. Am J Gastroenterol. 1992;87(3):337–41.
Bonavina L, Chirica M, Skrobic O, Kluger Y, Andreollo NA, Contini S, et al. Foregut caustic injuries: results of the world society of emergency surgery consensus conference. World J Emerg Surg. 2015;10:44.
Zargar SA, Kochhar R, Mehta S, Mehta SK. The role of fiberoptic endoscopy in the management of corrosive ingestion and modified endoscopic classification of burns. Gastrointest Endosc. 1991;37(2):165–9.
Cabral C, Chirica M, de Chaisemartin C, Gornet JM, Munoz-Bongrand N, Halimi B, et al. Caustic injuries of the upper digestive tract: a population observational study. Surg Endosc. 2012;26(1):214–21.
Alipour Faz A, Arsan F, Peyvandi H, Oroei M, Shafagh O, Peyvandi M, et al. Epidemiologic Features and Outcomes of Caustic Ingestions; a 10-Year Cross-Sectional Study. Emerg (Tehran). 2017;5(1):e56.
Ramasamy K, Gumaste VV. Corrosive ingestion in adults. J Clin Gastroenterol. 2003;37(2):199–24.
Javed A, Pal S, Krishnan EK, Sahni P, Chattopadhyay TK. Surgical management and outcomes of severe gastrointestinal injuries due to corrosive ingestion. World J Gastrointest Surg. 2012;4(5):121–5.
Lu LS, Tai WC, Hu ML, Wu KL, Chiu YC. Predicting the progress of caustic injury to complicated gastric outlet obstruction and esophageal stricture, using modified endoscopic mucosal injury grading scale. Biomed Res Int. 2014;2014:919870.
Le Naoures P, Hamy A, Lerolle N, Métivier E, Lermite E, Venara A. Risk factors for symptomatic esophageal stricture after caustic ingestion-a retrospective cohort study. Dis Esophagus. 2017;30(6):1–6.
Topaloglu B, Bicakci U, Tander B, Ariturk E, Kilicoglu-Aydin B, Aydin O, et al. Biochemical and histopathologic effects of omeprazole and vitamin E in rats with corrosive esophageal burns. Pediatr Surg Int. 2008;24(5):555–60.
Cakal B, Akbal E, Köklü S, Babalı A, Koçak E, Taş A. Acute therapy with intravenous omeprazole on caustic esophageal injury: a prospective case series. Dis Esophagus. 2013;26(1):22–6.
Arisawa T, Harata M, Kamiya Y, Shibata T, Nagasaka M, Nakamura M, et al. Is omeprazole or misoprostol superior for improving indomethacin-induced delayed maturation of granulation tissue in rat gastric ulcers? Digestion. 2006;73(1):32–9.
Biswas K, Bandyopatdhyay U, Chattopadyay I, Varadaraj A. A novel antioxidant and anti-apoptotic role of omeprazole to block gastric ulcer through scavenging of hydroxyl radical. J Biol Chem. 2003;278(13):10993–1001.
Kil BJ, Kim IW, Shin CY, Jeong JH, Jun CH, Lee SM, et al. Comparison of IY81149 with omeprazole in rat reflux oesophagitis. J Auton Pharmacol. 2000;20(5–6):291–6.
Kim YJ, Lee JS, Hong KS, Chung JW, Kim JH, Hahm KB. Novel application of proton pump inhibitor for the prevention of colitis-induced colorectal carcinogenesis beyond acid suppression. Cancer Prev Res (Phila). 2010;3(8):963–74.
Kobayashi T, Ohta Y, Inui K, Yoshino J, Nakazawa S. Protective effect of omeprazole against acute gastric mucosal lesions induced by compound 48/80, a mast cell degranulator, in rats. Pharmacol Res. 2002;46(1):75–84.
Pozzoli C, Menozzi A, Grandi D, Solenghi E, Ossiprandi MC, Zullian C, et al. Protective effects of proton pump inhibitors against indomethacin-induced lesions in the rat small intestine. Naunyn Schmiedebergs Arch Pharmacol. 2007;374(4):283–91.
Acknowledgments
The authors would like to thank staff members of Department of Surgery, Faculty of Medicine, Thammasat University, for the data of this study and special thanks to Norman Mangnall for assistance in editing the English version of this manuscript.
Author information
Authors and Affiliations
Contributions
All of the author and co-author listed: Prasit Mahawongkajit, Prakitpunthu Tomtitchong, Nuttorn Boochangkool, Palin Limpavitayaporn, Amonpon Kanlerd, Chatchai Mingmalairak, Surajit Awsakulsutthi, and Chittinad Havanond, followed the guidelines of the International Committee of Medical Journal Editors (ICMJE); all of the author listed in this manuscript met the four criteria of the guidelines of the International Committee of Medical Journal Editors (ICMJE).
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Mahawongkajit, P., Tomtitchong, P., Boochangkool, N. et al. Risk Factors for Esophageal Stricture in Grade 2b and 3a Corrosive Esophageal Injuries. J Gastrointest Surg 22, 1659–1664 (2018). https://doi.org/10.1007/s11605-018-3822-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-018-3822-x