
Abstract
Purpose
Preventable readmissions represent a major burden on the health care system and risk stratification of patients can help direct costly resources. This study examines patient characteristics, surgical factors, and postoperative complications associated with 30-day postoperative readmissions in gastrointestinal (GI) resections.
Methods
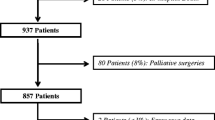
Inpatients undergoing major GI surgery were selected from the 2011 American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. Resections were classified into foregut, small bowel, colorectal, liver, and pancreatic using Current Procedural Terminology (CPT) codes. Postoperative complications were divided into pre- and post-discharge groups using time to complication and discharge. Univariate analysis compared patient and surgical characteristics and pre-discharge complications with 30-day unplanned readmission rates. Factors with a p value <0.1 were included in multivariate logistic regression. A p value <0.05 was considered statistically significant.
Results
For 42,609 patients undergoing GI resection, the overall 30-day unplanned readmission rate was 12.3 % ranging from 11.8 % for colorectal resections to 16.3 % for pancreatic resections. Major predictors of 30-day readmissions included pre-discharge major complications (odds ratio [OR] = 1.28, 95 % confidence interval [CI] 1.18–1.39, p < 0.0001), chronic steroid use (OR = 1.67, 95 % CI 1.50–1.86, p < 0.0001), operative time ≥4 h (OR = 1.45, 95 % CI 1.35–1.56, p < 0.0001) and discharge to a facility other than home (OR = 1.37, 95 % CI 1.23–1.50, p < 0.0001).
Conclusions
Unplanned 30-day readmissions represent a major clinical and financial concern, but some may be foreseeable and potentially modifiable. This model provides insight into factors that could inform resource utilization and postoperative care to help prevent readmissions in select GI surgical patients.
Similar content being viewed by others


References
Anderson GF, Steinberg EP: Hospital readmissions in the Medicare population. The New England journal of medicine 311(21), 1349–1353 (1984).
Fisher ES, Wennberg JE, Stukel TA, Sharp SM: Hospital readmission rates for cohorts of Medicare beneficiaries in Boston and New Haven. The New England journal of medicine 331(15), 989–995 (1994).
Jencks SF, Williams MV, Coleman EA: Rehospitalizations among patients in the Medicare fee-for-service program. The New England journal of medicine 360(14), 1418–1428 (2009).
Kelly M, Sharp L, Dwane F, Kelleher T, Comber H: Factors predicting hospital length-of-stay and readmission after colorectal resection: a population-based study of elective and emergency admissions. BMC health services research 12, 77 (2012).
Faiz O, Haji A, Burns E, Bottle A, Kennedy R, Aylin P: Hospital stay amongst patients undergoing major elective colorectal surgery: predicting prolonged stay and readmissions in NHS hospitals. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland 13(7), 816–822 (2011).
O'Brien DP, Senagore A, Merlino J, Brady K, Delaney C: Predictors and outcome of readmission after laparoscopic intestinal surgery. World journal of surgery 31(12), 2430–2435 (2007).
Kiran RP, Delaney CP, Senagore AJ, Steel M, Garafalo T, Fazio VW: Outcomes and prediction of hospital readmission after intestinal surgery. Journal of the American College of Surgeons 198(6), 877–883 (2004).
Schneider EB, Hyder O, Brooke BS et al.: Patient readmission and mortality after colorectal surgery for colon cancer: impact of length of stay relative to other clinical factors. Journal of the American College of Surgeons 214(4), 390–398; discussion 398–399 (2012).
Greenblatt DY, Weber SM, O'Connor ES, Loconte NK, Liou JI, Smith MA: Readmission after colectomy for cancer predicts one-year mortality. Annals of surgery 251(4), 659–669 (2010).
Wick EC, Shore AD, Hirose K et al.: Readmission rates and cost following colorectal surgery. Diseases of the colon and rectum 54(12), 1475–1479 (2011).
Kassin MT, Owen RM, Perez SD et al.: Risk factors for 30-day hospital readmission among general surgery patients. Journal of the American College of Surgeons 215(3), 322–330 (2012).
Kariv Y, Wang W, Senagore AJ, Hammel JP, Fazio VW, Delaney CP: Multivariable analysis of factors associated with hospital readmission after intestinal surgery. American journal of surgery 191(3), 364–371 (2006).
Hendren S, Morris AM, Zhang W, Dimick J: Early discharge and hospital readmission after colectomy for cancer. Diseases of the colon and rectum 54(11), 1362–1367 (2011).
Ahmad SA, Edwards MJ, Sutton JM: Factors influencing readmission after pancreaticoduodenectomy: a multi-institutional study of 1302 patients. Annals of surgery 256(3), 529–537 (2012).
Reddy DM, Townsend CM, Jr., Kuo YF, Freeman JL, Goodwin JS, Riall TS: Readmission after pancreatectomy for pancreatic cancer in Medicare patients. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract 13(11), 1963–1974; discussion 1974–1965 (2009).
Kent TS, Sachs TE, Callery MP, Vollmer CM, Jr.: Readmission after major pancreatic resection: a necessary evil? Journal of the American College of Surgeons 213(4), 515–523 (2011).
Weiss AJ, Elixhauser A, Steiner C: Readmissions to U.S. hospitals by procedure in 2010. HCUP Statistical Brief #154, (2013).
Barbas AS, Turley RS, Mallipeddi MK et al.: Examining reoperation and readmission after hepatic surgery. Journal of the American College of Surgeons 216(5), 915–923 (2013).
Lawson EH, Hall BL, Louie R et al.: Association between occurrence of a postoperative complication and readmission: implications for quality improvement and cost savings. Annals of surgery 258(1), 10–18 (2013).
Khuri SF: The NSQIP: a new frontier in surgery. Surgery 138(5), 837–843 (2005).
Fleming FJ, Francone TD, Kim MJ, Gunzler D, Messing S, Monson JR: A laparoscopic approach does reduce short-term complications in patients undergoing ileal pouch–anal anastomosis. Diseases of the colon and rectum 54(2), 176–182 (2011).
ACS NSQIP: Inclusion/Exclusion Criteria http://site.acsnsqip.org/program-specifics/inclusionexclusion-criteria-4/ . (4/13/2013),
Gabbert W, Kachur K, Canter K: Current Procedural Coding Expert 2011. Ingenix, USA. (2010).
Messaris E, Sehgal R, Deiling S et al.: Dehydration is the most common indication for readmission after diverting ileostomy creation. Diseases of the colon and rectum 55(2), 175–180 (2012).
Sharma A, Deeb AP, Iannuzzi JC, Rickles AS, Monson JR, Fleming FJ: Tobacco smoking and postoperative outcomes after colorectal surgery. Annals of surgery 258(2), 296–300 (2013).
Mills E, Eyawo O, Lockhart I, Kelly S, Wu P, Ebbert JO: Smoking cessation reduces postoperative complications: a systematic review and meta-analysis. The American journal of medicine 124(2), 144–154 e148 (2011).
Emick DM, Riall TS, Cameron JL et al.: Hospital readmission after pancreaticoduodenectomy. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract 10(9), 1243–1252; discussion 1252–1243 (2006).
Vashi AA, Fox JP, Carr BG et al.: Use of hospital-based acute care among patients recently discharged from the hospital. JAMA : the journal of the American Medical Association 309(4), 364–371. (2013).
Sellers MM, Merkow RP, Halverson A et al.: Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. Journal of the American College of Surgeons 216(3), 420–427 (2013).
Hechenbleikner EM, Makary MA, Samarov DV et al.: Hospital readmission by method of data collection. Journal of the American College of Surgeons 216(6), 1150–1158 (2013).
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussant
Dr. Taylor Riall (Galveston, Texas): Dr. Kelly, I congratulate you on an excellent presentation. With looming changes in Medicare policy regarding reimbursement for readmissions after surgery, it is critical that we, as surgeons, understand the root cause of these readmissions and identify potential targets for intervention and improvement.
We all strive to lower complication rates. However, given the complexity of what we do, we recognize that a 30-day readmission rate of zero is likely not feasible. Based on your data, it seems to me there are two real opportunities for intervention. The first is better recognition and management with regard to post-discharge complications. You report approximately 2,700 complications that occurred post-discharge, with a nearly 60-fold increase in the odds of readmission in this group. This may be an artifact of your methodology — as you demonstrate, patients experiencing post-discharge complications had shorter lengths of stay, and therefore, longer time "at risk" for readmission based on the NSQIP definition of 30 days from surgery. Do you think that these complications are unrecognized at the time of discharge? Are patients are discharged to early? For example, are patients being discharged with a slightly increasing WBC despite no fever with a smoldering infection? It would be interesting to look back on patients who develop post-discharge infections and see if there were subtle signs prior to discharge.
The second opportunity is improving postoperative follow-up. I know you can't do this with NSQIP, but you may be able to do this with other datasets. It would be interesting to evaluate postoperative visits to the operating surgeon and/or primary care physician between discharge and readmission — both if and when they occurred. I suspect that postoperative follow-up would be less adequate in patients requiring readmission. Systems-level interventions to improve surgeon follow-up, may increase recognition and decrease the impact of post-discharge infections on readmission. Since a significant proportion of readmissions seemed unrelated to documented operative complications, PCP follow-up might decrease readmissions related to exacerbations of chronic illness. And, while you argue that discharge to skilled nursing facility is a "non-modifiable" risk factor, I would disagree. I think better communication of the plan, expected course, and management of drains, etc. would decrease readmissions from SNFs. How do you communicate with SNFs after patient discharge? How early do you see patients back? Do you ensure PCP follow-up as well? Have you put any systems in place to address these issues?
Again, I congratulate Dr. Kelly on an excellent presentation and manuscript.
Closing Discussant
Dr. Kristin Kelly: I would like to thank Dr. Riall for some very interesting thoughts and questions. She has truly captured many of the important issues and challenges we face in trying to better understand surgical readmissions as a means of improving patient care and postoperative outcomes.
To her first point regarding postoperative complications and the timing of interventions, we agree there are really two opportunities for potential intervention. The first opportunity for intervention, that Dr. Riall highlighted, is in developing better, earlier means to identify which patients are at risk for later postoperative complications. Not surprisingly, patients who experience a major complication at home after discharge almost inevitably and appropriately return to the hospital. In an age of decreasing length of stay and more protocolized postoperative care there may be a few patients whose subtle signs of early infection or future complications are missed, but arguably many patients are probably at home well before any indication of trouble is present. In our study patients with post-discharge complications returned to the hospital a mean 7–10 days after discharge, so keeping them for an extra day or two probably would not have significantly impacted their clinical course. Certainly keeping patients an extended time is not clinically or fiscally practical. To date, no literature has explored in depth our ability to predict these postoperative complications and moving forward this will probably be a very critical area to study for directing interventions to address this opportunity.
The second opportunity occurs in recognizing the increased risk of subsequent complications and readmissions in patients who have a major complication prior to discharge. These patients remain in the hospital for longer periods of time meaning they have less "at risk" time at home for readmission based upon NSQIP's 30-day definition, but interestingly we still find that they have an increased risk of readmission compared to patients who did not have a major complication before discharge. These patients would likely benefit from close outpatient monitoring or early improved follow-up with attention to any barriers or challenges they may face during the transition home. We agree with Dr. Riall that studying and improving the systems in place for discharge and postoperative follow-up will likely decrease readmission rates in patients who currently have unmet needs after discharge.
The issue regarding skilled nursing facilities after discharge is a complex one. We initially classified this variable as non-modifiable from the standpoint that there is likely little that can be done at the time of surgery to change the patient's comorbidities, functional status, social support, or other factors driving the need for skilled nursing after discharge. While we may not have the ability to impact the requirement for a nursing facility, we do agree with the point that improving the communication with these facilities could be a targetable point of intervention. This might be achieved by working with the SNFs to increase the understanding of common postoperative surgical issues and warning signs or by calling the physicians responsible for SNF patients at the time of discharge to ensure open lines of communication. Currently the system is not formally structured to ensure this valuable communication. Timely follow-up appointments with the PCP and surgeon, the discussion of any critical information, and conveying any changes in chronic illness as a result of surgery depend upon the initiative and preferences of individual providers. If SNFs are considered from this perspective, then there are most certainly modifiable targets for improving readmission rates in this at risk population.
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Kelly, K.N., Iannuzzi, J.C., Rickles, A.S. et al. Risk Factors Associated with 30-Day Postoperative Readmissions in Major Gastrointestinal Resections. J Gastrointest Surg 18, 35–44 (2014). https://doi.org/10.1007/s11605-013-2354-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-013-2354-7