
Abstract
Introduction
Incidental pulmonary nodules are frequently identified during staging investigations for esophageal cancer patients. Their clinical significance is unclear and may bias treatment decisions towards palliative options.
Methods
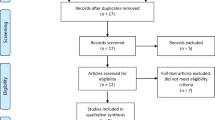
From 2005 to 2011, 423 esophageal cancer patients were treated at a tertiary hospital. Those with incidental pulmonary nodules were identified. Demographics, imaging, pathology and perioperative outcomes were analyzed.
Results
Ninety-two patients (22 %) had lung nodules. Twenty-nine (32 %) were palliative due to poor performance status or extra-pulmonary distant metastasis on imaging. Sixty-three had no evidence of extra-pulmonary metastasis and underwent curative-intent treatment comprising of neoadjuvant therapy [35 (55 %)] followed by esophagectomy [with lung resection, 33 (52 %) or without lung resection, 30 (48 %)]. Of those 33 lung resections, there were 27 benign lesions, 4 stage I lung cancers, and 1 esophageal cancer metastasis. Of 30 patients with lung nodules that underwent curative esophagectomy without lung resection, none showed interval size increase on follow-up imaging [median 9 months (3–40)]. There was no difference in perioperative complications or mortality between patients with combined esophagectomy and lung resection and those with esophagectomy alone.
Conclusion
Incidental pulmonary nodules in the absence of extra-pulmonary metastases in esophageal cancer patients are rarely metastases and should not bias caregivers towards palliative therapy.

Similar content being viewed by others


References
Pennathur, A., et al., Oesophageal carcinoma. Lancet, 2013. 381(9864): p. 400–12.
Ferlay, J., et al., Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer, 2010. 127(12): p. 2893–917.
Jemal, A., et al., Cancer statistics, 2009. CA Cancer J Clin, 2009. 59(4): p. 225–49.
Lepage, C., et al., Continuing rapid increase in esophageal adenocarcinoma in England and Wales. Am J Gastroenterol, 2008. 103(11): p. 2694–9.
Quint, L.E., et al., Incidence and distribution of distant metastases from newly diagnosed esophageal carcinoma. Cancer, 1995. 76(7): p. 1120–5.
Sons, H.U. and F. Borchard, Cancer of the distal esophagus and cardia. Incidence, tumorous infiltration, and metastatic spread. Ann Surg, 1986. 203(2): p. 188–95.
Anderson, L.L. and T.E. Lad, Autopsy findings in squamous-cell carcinoma of the esophagus. Cancer, 1982. 50(8): p. 1587–90.
Chan, K.W., E.Y. Chan, and C.W. Chan, Carcinoma of the esophagus. An autopsy study of 231 cases. Pathology, 1986. 18(4): p. 400–5.
Bosch, A., et al., Autopsy findings in carcinoma of the esophagus. Acta Radiol Oncol Radiat Phys Biol, 1979. 18(2): p. 103–12.
Mandard, A.M., et al., Autopsy findings in 111 cases of esophageal cancer. Cancer, 1981. 48(2): p. 329–35.
Margolis, M.L., P. Howlett, and R. Bubanj, Pulmonary nodules in patients with esophageal carcinoma. J Clin Gastroenterol, 1998. 26(4): p. 245–8.
van Westreenen, H.L., et al., Synchronous primary neoplasms detected on 18F-FDG PET in staging of patients with esophageal cancer. J Nucl Med, 2005. 46(8): p. 1321–5.
Clavien, P.A., et al., The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg, 2009. 250(2): p. 187–96.
Clavien, P.A., J.R. Sanabria, and S.M. Strasberg, Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery, 1992. 111(5): p. 518–26.
Dindo, D., N. Demartines, and P.A. Clavien, Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg, 2004. 240(2): p. 205–13.
American Joint Committee on Cancer Staging Manual. 7 ed, ed. B.D. Edge SB, Compton CC, Fritz AG, Greene FL, Trotti A 2010, New York: Springer.
Ferri, L.E., et al., Perioperative docetaxel, cisplatin, and 5-fluorouracil (DCF) for locally advanced esophageal and gastric adenocarcinoma: a multicenter phase II trial. Ann Oncol, 2012. 23(6): p. 1512–7.
Gohagan, J., et al., Baseline findings of a randomized feasibility trial of lung cancer screening with spiral CT scan vs chest radiograph: the Lung Screening Study of the National Cancer Institute. Chest, 2004. 126(1): p. 114–21.
Swensen, S.J., et al., Lung cancer screening with CT: Mayo Clinic experience. Radiology, 2003. 226(3): p. 756–61.
van Westreenen, H.L., et al., Positron emission tomography with F-18-fluorodeoxyglucose in a combined staging strategy of esophageal cancer prevents unnecessary surgical explorations. J Gastrointest Surg, 2005. 9(1): p. 54–61.
Zhu, Y., et al., Simultaneous operation of concomitant diseases in the esophagus and lung. Dis Esophagus, 2011. 24(4): p. 279–82.
Wang, X.X., et al., Is surgical treatment of cancer of the gastric cardia or esophagus associated with a concurrent major pulmonary operation feasible? One center's experience. Chin Med J (Engl), 2012. 125(2): p. 193–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussant
Dr. John Hunter (Portland, Oregon): This is a paper that can change the care of the patient with esophageal cancer, many of whom have small pulmonary nodules. What it tells us is that small pulmonary nodules, <1 cm in diameter are highly likely to be benign and should not influence or alter the care pathways of patients with locally advanced esophageal cancer. In fact, the most common malignant diagnosis for such nodules is primary lung cancer, not esophageal cancer and all of these were > 1 cm in size. The clever thing that this group did was to remove the small nodules in the right lung, proving the benign nature of these lesions and left the sub-centimeter nodules in the left lung alone, giving them the test of time to prove that they were not malignant.
In this era of multimodality therapy, many of these patients have the benefit of receiving more than one chest CT before they come to resection. Given this paradigm, it is clear that lesions over 1 cm and those that are growing over a 3-month period should be biopsied before esophagectomy. Those that are not growing are probably benign, especially if less than 1 cm in size. Those that shrink or go away are more problematic, especially if they are too small to find at the time of referral or esophagectomy. Are these “shrinking” lesions lung metastases responding to chemoradiotherapy? Are they inflammatory? Three questions:
1. What do you do when you see several suspicious pulmonary lesions that were not biopsied initially but have now shrunk on chemo to a size no longer able to be biopsied percutaneously?
2. For suspicious right lung lesions, I imagine you address them at the time of thoracotomy or thoracoscopy. What criteria would push you to biopsy or resect a left lung nodule on another occasion in anticipation of esophagectomy?
3. When a primary lung cancer is detected on CT staging for esophageal cancer, what should you do? Address the lung cancer before neoadjuvant esophageal cancer treatment? Address the lung cancer at the time of esophagectomy? And what would you do if the apparent lung cancer is in the left lung?
Many thanks for the chance to look at the manuscript it advance. Good work.
Closing Discussant
Dr. Amin Madani: Dear Dr. Hunter, thank you for your insightful comments.
1. What do you do when you see several suspicious pulmonary lesions that were not biopsied initially but have now shrunk on chemo to a size no longer able to be biopsied percutaneously?
As you mentioned, it is difficult to ascertain the etiology of lung nodules that have shrunk or are no longer detectable on repeat imaging post-neoadjuvant chemotherapy. Indeed, there were 30 patients with lung nodules less than 1 cm for whom we did not obtain pathologic confirmation. The question then becomes, how do we know if these lesions harbored a malignancy? Firstly, only half of them received chemotherapy. Secondly, follow-up imaging was done postoperatively until a median of 9 months (range 3–40), not just after neoadjuvant chemotherapy, giving the nodule time for growth were it truly a malignant lesion. The fact that there was no growth interval of the nodules in this time frame makes it very unlikely to be malignant. More importantly, there were 25 patients with sub-centimetric nodules for whom we have pathologic confirmation of their benign nature. Most of these happen to be inflammatory or infectious, which is not surprising, given these patients' propensity to aspirate from an obstructing mass. Therefore, if a patient with esophageal cancer is found to have pulmonary nodules, without evidence of extra-thoracic metastasis, they should still be offered curative-intent therapy–—despite having undergone chemotherapy and despite the lesions' inaccessibility to percutaneous biopsy.
2. For suspicious right lung lesions, I imagine you address them at the time of thoracotomy or thoracoscopy. What criteria would push you to biopsy or resect a left lung nodule on another occasion in anticipation of esophagectomy?
If the lung nodule happens to be in a contralateral location to where the esophagectomy is planned, repeat imaging can be used to the clinician's advantage, both after neoadjuvant chemotherapy and again postoperatively. If suspicion for a primary lung malignancy still exists, then appropriate diagnostic modalities such as CT-guided biopsy or endoscopic ultrasound biopsy should be undertaken followed by the appropriate therapeutic intervention. The four primary malignancies in our cohort were all stage I. Therefore, surgical resection of these lung nodules was likely curative.
3. When a primary lung cancer is detected on CT staging for esophageal cancer, what should you do? Address the lung cancer before neoadjuvant esophageal cancer treatment? Address the lung cancer at the time of esophagectomy? And what would you do if the apparent lung cancer is in the left lung?
An uncommon but complex scenario is when two primary malignancies exist. Ideally, two multidisciplinary teams specialized in each malignancy should review the case and coordinate together a therapeutic plan, where the malignancy with the gravest prognosis takes precedence. In the case of concomitant primary lung and esophageal malignancies, it would be the esophageal cancer. In many instances, both are amenable to surgery and all efforts should be made at providing oncologically sound en bloc resections. If the lung cancer is in the ipsilateral location to the thoracic approach of the esophagectomy, it can be resected with minimal difficulty at the time of the esophagectomy. However, if it is located in a contralateral location, the lung cancer can be resected following successful recovery from the esophagectomy. If the lung resection is amenable to minimally invasive thoracoscopic techniques, it may also be feasible to be done at the time of the esophagectomy. Ultimately, all cases are unique and a well-coordinated plan should be devised and catered to each patient by a multidisciplinary team.
Thank you for taking the time to review our manuscript.
This manuscript was presented as a plenary lecture presentation at The Society for Surgery of the Alimentary Tract 54th Annual Meeting, Orlando, Florida, on May 21, 2013.
This manuscript was awarded the 2013 Society for Surgery of the Alimentary Tract Residents and Fellows Research Conference Award.
Rights and permissions
About this article
Cite this article
Madani, A., Spicer, J., Alcindor, T. et al. Clinical Significance of Incidental Pulmonary Nodules in Esophageal Cancer Patients. J Gastrointest Surg 18, 226–233 (2014). https://doi.org/10.1007/s11605-013-2339-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-013-2339-6