
Abstract
Objective
The objective of the study was to analyze surgical site infection (SSI) frequency with different duration antibiotic courses to establish the minimum necessary duration.
Methods
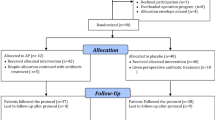
This is an observational study of prospective surveillance of 287 consecutive patients (mean age 67.8 years) operated on for acute cholecystitis of grade II severity in the first 72 h. Postoperative antibiotics had been withdrawn before diagnosis of any infection as an inclusion criterion. Patients were classified into three groups, according to therapy duration: group 1 (0–4 days, n = 45, 15.7 %); group 2 (5–7 days, n = 75, 26.1 %); and group 3 (>7 days, n = 167, 58.2 %). A multivariable analysis of risk infection was performed.
Results
Overall SSI frequency in groups 1, 2, and 3 was 2.2, 10.7, and 9 %, respectively. Risk analysis showed an increase in both crude and adjusted relative risks of overall infection in group 2 (crude relative risk (RR): 4.80 (0.62–37.13); adjusted RR, 2.03 (0.20–20.91)) and in group 3 (crude RR, 4.04 (0.55–29.79); adjusted RR, 2.35 (0.28–20.05)) by comparison with group 1, although without statistical significance. As a result, treatment lasting 4 days or less was not associated with overall surgical site infection incidence higher than longer treatment.
Conclusion
Antibiotic treatment over 4 days after early cholecystectomy provides no advantage in decreasing surgical site infection incidence.
Similar content being viewed by others


References
Yoshida M, Takada T, Kawarada Y, Tanaka A, Nimura Y, Gomi H, Hirota M, Miura F, Wada K, Mayumi T, Solomkin JS, Strasberg S, Pitt HA, Belghti J, de Santibanes E, Fan ST, Chen MF, Belli G, Hilvano SC, Kim SW, Ker CG. Antimicrobial therapy for acute cholecystitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg 2007; 14: 83–90
Gomi A, Solomkin JS, Takada T, Strasberg SM, Pitt HA, Yoshida M, Kusachi S, Mayumi T, Miura F, Kiriyama S, Yokoe M, Kimura Y, Higuchi R, Windsor JA, Dervenis C, Liau KH, Kim MH. TG13 antimicrobial therapy for acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci 2013; 20: 60–70
Strasberg SM. Acute Calculous Cholecystitis. N Eng J Med 2008; 358: 2804–11
Kanafani, ZA, Khalifé N, Kanj SS, Araj GF, Khalifeh M, Sharara AI. Antibiotic use in acute cholecystitis: practice patterns in the absence of evidence-based guidelines. J Infect 2005; 51: 128–134
Lau WY, Yuen WK, Chu KW, Chong KK, Li AK. Systemic antibiotic regimens for acute cholecystitis treated by early cholecystectomy. Aust N Z J Surg 1990; 60: 539–43
Kune GA, Burdon JG. Are antibiotics necessary in acute cholecystitis? Med J Aust 1975; 2: 627–30
Guirao X, Arias J, Badía JM, García-Rodríguez JA, Mensa J, Álvarez-Lerma F, Borges M, Barberán J, Maseda M, Salavert M, Llinares P, Gobernadó M, García Rey C. Recomendaciones en el tratamiento antibiótico empírico de la infección intraabdominal. Cir Esp 2010; 87: 63–81
Solomkin JS, Mazuski JE, Baron EJ, Sawyer RG, Nathens AB, DiPiro JT et al. Guidelines for the selection of anti-infective agents for complicated intra-abdominal infections. Clin Infect Dis 2003; 37: 997–1005
Yokoe M, Takada T, Strasberg SM, Solomkin JS, Mayumi T, Gomi H, Pitt HA, Garden OJ, Kiriyama S, Gouma DJ, Garden OJ, Büchler MW, Kiriyama S, Hata J, Gabata T, Yoshida M, Miura F, Okamoto K, Tsuyuguchi T, Itoi T, Yamashita Y, Dervenis C, Chan ACW, Lau WY, Supe AN, Belli G, Hilvano SC, Liau KH, Kim MH, Kim SH, Ker CG. TG13 diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci 2013; 20: 35–46
Little JP. Consistency of ASA grading. Anaesthesia 1995; 50: 658–659
Culver DH, Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG, Banerjee SN, Edwuards JR, Tolson JS, Henderson TS, Hughes JM, National Nosocomial Infections surveillance system. Surgical wound infection rates by wound class, operative procedure, and patient risk index. Am J Med 1991; 91 (Suppl 2): 152S–157S
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008; 36: 309–332
Mazeh H, Mizrahi I, Dior U, Simanovsky N, Shapiro M, Freund HR, Eid A. Role of antibiotics in mild acute calculous cholecystitis: A prospective randomized controlled trial. World J Surg 2012: 36: 1750–9
Papi C, Catarci M, D'Ambrosio L, Gili L, Koch M, Grassi GB, Capurso L. Timing of cholecystectomy for acute calculous cholecystitis: A meta-analysis. Am J Gastroenterol 2004; 99: 147–155
Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Cochrane Database Syst Rev. 2006 Oct 18; (4):CD005440.
Thompson JE, Bennion RS, Doty JE, Muller EL, Pitt HA. Predictive factors for bactibilia in acute cholecystitis. Arch Surg 1990; 125: 261–264
Galili O, Eldar S Jr, Matter I, Madi H, Brodsky A, Galis I, Eldar S Sr. The effect of bactibilia on the course and outcome of laparoscopic cholecystectomy. Eur J Clin Microbiol Infect Dis. 2008; 27: 797–803
Author information
Authors and Affiliations
Corresponding author
Additional information
The study was approved by the local Committee of ethics in Clinical Research.
Rights and permissions
About this article
Cite this article
Rodríguez-Sanjuán, J.C., Casella, G., Antolín, F. et al. How Long Is Antibiotic Therapy Necessary After Urgent Cholecystectomy for Acute Cholecystitis?. J Gastrointest Surg 17, 1947–1952 (2013). https://doi.org/10.1007/s11605-013-2321-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-013-2321-3