
Abstract
Introduction
There has been increased attention focused on reducing postoperative length of stay and mortality following colorectal surgery. We sought to identify adverse events associated with prolonged length of stay and mortality.
Methods
We evaluated postoperative “adverse events,” prolonged length of stay, and mortality within 30 days of colorectal surgery in the National Surgical Quality Improvement Program (NSQIP) hospitals from January 2005 through December 2008. We then used multivariate models to establish the associations between adverse events and prolonged length of stay and mortality.
Results
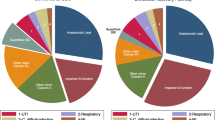
A total of 54,237 patients underwent colorectal surgery: 39,980 (74 %) experienced no postoperative adverse events, while 14,257 (26 %) experienced one or more adverse events. Length of stay was prolonged (longer than 10 days) in 38 % of patients who experienced a postoperative adverse event and in 15 % of patients without events. Mortality increased with the number of postoperative adverse events. In multivariate models including preoperative comorbidity, patient risk factors, and adverse events, patients who experienced a cardiac arrest, septic shock, stroke, myocardial infarction, and/or renal failure were at highest odds of dying within 30 days of surgery.
Conclusions
Patients with cardiac arrest, septic shock, stroke, myocardial infarction, and/or renal failure are at highest risk of mortality following colorectal surgery.
Similar content being viewed by others


References
Khuri SF, Daley J, Henderson W, Hur K, Demakis J, Aust JB, Chong V, Fabri PJ, Gibbs JO, Grover F, Hammermeister K, Irvin G 3rd, McDonald G, Passaro E Jr, Phillips L, Scamman F, Spencer J, Stremple JF. The Department of Veterans Affairs’ NSQIP: The first national, validated, outcome-based, risk-adjusted, and peer-controlled program for the measurement and enhancement of the quality of surgical care. National VA Surgical Quality Improvement Program. Ann Surg. 1998;228:491–507.
Schilling PL, Dimick JB, Birkmeyer JD. Prioritizing quality improvement in general surgery. J Am Coll Surg. 2008;207:698–704.
American College of Surgeons National Surgical Quality Improvement Program. ACS NSQIP. Available at: www.acsnsqip.org/main/programspecs/program_data_collection.jsp Accessed November 14, 2010.
Beyond the HIPAA privacy rule: enhancing privacy, improving health through research. Institute of Medicine (US) Committee on Health Research and the Privacy of Health Information: The HIPAA Privacy Rule; Nass SJ, Levit LA, Gostin LO, editors. Washington, DC: National Academies Press (US); 2009.
Rowell KS, Turrentine FE, Hutter MM, Khuri SF, Henderson W. Use of National Surgical Quality Improvement Program data as a catalyst for quality improvement. J Am Coll Surg. 2007;204:1293–1300.
ACS NSQIP data: participant use data file. American College of Surgeons National Surgical Quality Improvement Program Web site. Available at: www.acsnsqip.org/puf/PufRequestHomepage.aspx. Accessed May 20, 2010.
Cohen ME, Bilimoria KY, Ko CY, Richards K, Hall BL. Variability in length of stay after colorectal surgery: assessment of 182 hospitals in the National Surgical Quality Improvement Program. Ann Surg. 2009;250:901–7.
Ingraham AM, Cohen ME, Bilimoria KY. Comparison of hospital performance in nonemergency versus emergency colorectal operations at 142 hospitals. J Am Coll Surg. 2010;210:155–165.
American College of Surgeons. American College of Surgeons National Surgical Quality Improvement Program Operations Manual. Available at: www.registry.acsnsqip.org/codingInstructions.html. Accessed Nov 22, 2010.
Iyer S, Saunders WB, Stemkowski S. Economic burden of postoperative ileus associated with colectomy in the United States. J Manag Care Pharm. 2009;15:485–494.
Swenson BR, Hollenbeak CS, Koltun WA. Factors affecting cost and length of stay associated with the ileal pouch-anal anastomosis. Dis Colon Rectum. 2003;46:754–761.
McAleese P, Odling-Smee W. The effect of complications on length of stay. Ann Surg. 1994;220:740–4.
Tess BH, Glenister HM, Rodrigues LC, Wagner MB. Incidence of hospital-acquired infection and length of hospital stay. Eur J Clin Microbiol Infect Dis. 1993;12:81–86.
National Quality Measures Clearinghouse. Surgical Care Improvement Project Available at: http://qualitymeasures.ahrq.gov/browse/by-organization-indiv.aspx?objid=13239 Accessed July 25, 2011.
Gold JH. The Surgical Care Improvement Project. Wisconsin Medical Journal. 2005;104:73–74.
Bratzler DW, Hunt DR. The surgical infection prevention and surgical care improvement projects: national initiatives to improve outcomes for patients having surgery. Clin Infect Dis. 2006;43:322–330.
American College of Surgeons: Continuous Quality Improvement: Program Overview. Available at: http://www.facs.org/cqi/outcomes.html Accessed August 8, 2011.
Brook RH. The end of the quality improvement movement. JAMA 2010;304:1831–1832.
Disclaimer
The ACS NSQIP and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. The study has been approved by all authors in the present format.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Segmental Colectomy: 44139, 44140, 44141, 44143, 44144, 44160, 44204, 44205, 44206, 44213, 45402, 45550
Proctectomy: 44207, 44208, 44145, 44146, 44147, 45111, 45112, 45113, 45114, 45116, 45119, 45120, 45123, 45130, 45135, 45397
Total Colectomy: 44150, 44151, 44210
Proctocolectomy: 44152, 44153, 44155, 44156, 44211, 44212, 44157, 44158, 45121
Abdominoperineal Resection: 45110, 45126, 45395
Rights and permissions
About this article
Cite this article
Ricciardi, R., Roberts, P.L., Read, T.E. et al. Which Adverse Events are Associated with Mortality and Prolonged Length of Stay Following Colorectal Surgery?. J Gastrointest Surg 17, 1485–1493 (2013). https://doi.org/10.1007/s11605-013-2224-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-013-2224-3