
Abstract
Introduction
Pancreatic intraductal papillary mucinous neoplasms (IPMN) are now identified with increasing frequency. The detection of carcinoma in IPMN is difficult and suffers from high false-positive and false-negative rates, often resulting in inappropriate treatment decisions. Improved detection of malignancy using novel biomarkers may therefore improve diagnostic accuracy. One such promising novel biomarker is Plectin-1 (Plec-1).
Methods
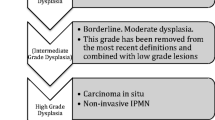
Using immunohistochemistry, Plec-1 expression was assayed in benign (low and moderate dysplasia, n = 6) as well as malignant IPMN (high-grade dysplasia and invasive carcinoma, n = 31) and lymph node metastases from carcinoma arising in IPMN (n = 12). Furthermore, cyst fluids from benign (n = 3) and malignant IPMN (n = 4) were evaluated for Plec-1 expression.
Results and discussion
Twenty-six of 31 malignant IPMN and all 12 lymph node metastases were Plec-1 positive. In contrast, only one of six benign IPMN expressed Plec-1. The specificity of Plec-1 in distinguishing malignant IPMN from benign IPMN was 83% and its sensitivity 84%. Furthermore, all (four out of four) cyst fluids from malignant IPMN, but none of the three benign IPMN, were Plec-1 positive. These data support Plec-1 as an excellent biomarker for the early detection of carcinoma arising in IPMN.


Similar content being viewed by others

References
Chari ST, Yadav D, Smyrk TC, DiMagno EP, Miller LJ, Raimondo M, Clain JE, Norton IA, Pearson RK, Petersen BT, Wiersema MJ, Farnell MB, Sarr MG. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology 2002;123:1500–1507.
Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M, Takeda K, Matsuno S, Furukawa T. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg 1999;134:1131–1136.
Salvia R, Fernandez-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, Pederzoli P, Warshaw AL. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg 2004;239:678–685. discussion 685–687.
Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N, Campbell KA, Lillemoe KD. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg 2004;239:788–797. discussion 797–9.
Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, Yamaguchi K, Yamao K, Matsuno S. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006;6:17–32.
Salvia R, Crippa S, Falconi M, Bassi C, Guarise A, Scarpa A, Pederzoli P. Branch-duct intraductal papillary mucinous neoplasms of the pancreas: to operate or not to operate? Gut 2007;56:1086–1090.
Bernard P, Scoazec JY, Joubert M, Kahn X, Le Borgne J, Berger F, Partensky C. Intraductal papillary-mucinous tumors of the pancreas: predictive criteria of malignancy according to pathological examination of 53 cases. Arch Surg 2002;137:1274–1278.
Yamao K, Ohashi K, Nakamura T, Suzuki T, Shimizu Y, Nakamura Y, Horibe Y, Yanagisawa A, Nakao A, Nimuara Y, Naito Y, Hayakawa T. The prognosis of intraductal papillary mucinous tumors of the pancreas. Hepatogastroenterology 2000;47:1129–1134.
Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006;244:10–15.
Richter A, Niedergethmann M, Sturm JW, Lorenz D, Post S, Trede M. Long-term results of partial pancreaticoduodenectomy for ductal adenocarcinoma of the pancreatic head: 25-year experience. World J Surg 2003;27:324–329.
Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Buchler MW. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg 2004;91:586–594.
Rodriguez JR, Salvia R, Crippa S, Warshaw AL, Bassi C, Falconi M, Thayer SP, Lauwers GY, Capelli P, Mino-Kenudson M, Razo O, McGrath D, Pederzoli P, Fernandez-Del Castillo C. Branch-duct intraductal papillary mucinous neoplasms: observations in 145 patients who underwent resection. Gastroenterology 2007;133:72–79. quiz 309–10.
Terris B, Ponsot P, Paye F, Hammel P, Sauvanet A, Molas G, Bernades P, Belghiti J, Ruszniewski P, Flejou JF. Intraductal papillary mucinous tumors of the pancreas confined to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol 2000;24:1372–1377.
Nagai K, Doi R, Ito T, Kida A, Koizumi M, Masui T, Kawaguchi Y, Ogawa K, Uemoto S. Single-institution validation of the international consensus guidelines for treatment of branch duct intraductal papillary mucinous neoplasms of the pancreas. J Hepatobiliary Pancreat Surg 2009;16:353–358.
Ogawa H, Itoh S, Ikeda M, Suzuki K, Naganawa S. Intraductal papillary mucinous neoplasm of the pancreas: assessment of the likelihood of invasiveness with multisection CT. Radiology 2008;248:876–886.
Sahani DV, Kadavigere R, Blake M, Fernandez-Del Castillo C, Lauwers GY, Hahn PF. Intraductal papillary mucinous neoplasm of pancreas: multi-detector row CT with 2D curved reformations—correlation with MRCP. Radiology 2006;238:560–569.
Pais SA, Attasaranya S, Leblanc JK, Sherman S, Schmidt CM, DeWitt J. Role of endoscopic ultrasound in the diagnosis of intraductal papillary mucinous neoplasms: correlation with surgical histopathology. Clin Gastroenterol Hepatol 2007;5:489–495.
Maire F, Voitot H, Aubert A, Palazzo L, O'Toole D, Couvelard A, Levy P, Vidaud M, Sauvanet A, Ruszniewski P, Hammel P. Intraductal papillary mucinous neoplasms of the pancreas: performance of pancreatic fluid analysis for positive diagnosis and the prediction of malignancy. Am J Gastroenterol 2008;103:2871–2877.
Wiesenauer CA, Schmidt CM, Cummings OW, Yiannoutsos CT, Howard TJ, Wiebke EA, Goulet RJ Jr., McHenry L, Sherman S, Lehman GA, Cramer H, Madura JA. Preoperative predictors of malignancy in pancreatic intraductal papillary mucinous neoplasms. Arch Surg 2003;138:610–617. discussion 617–8.
Pitman MB, Michaels PJ, Deshpande V, Brugge WR, Bounds BC. Cytological and cyst fluid analysis of small (< or =3 cm) branch duct intraductal papillary mucinous neoplasms adds value to patient management decisions. Pancreatology 2008;8:277–284.
Pelaez-Luna M, Chari ST, Smyrk TC, Takahashi N, Clain JE, Levy MJ, Pearson RK, Petersen BT, Topazian MD, Vege SS, Kendrick M, Farnell MB. Do consensus indications for resection in branch duct intraductal papillary mucinous neoplasm predict malignancy? A study of 147 patients. Am J Gastroenterol 2007;102:1759–1764.
Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushik N, Ahmad N, Brugge WR, Edmundowicz SA, Hawes RH, McGrath KM. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc 2009;69:1095–1102.
Kelly KA, Bardeesy N, Anbazhagan R, Gurumurthy S, Berger J, Alencar H, DePinho RA, Mahmood U, Weissleder R. Targeted nanoparticles for imaging incipient pancreatic ductal adenocarcinoma. PLoS Med 2008;5:e85.
Errante LD, Wiche G, Shaw G. Distribution of plectin, an intermediate filament-associated protein, in the adult rat central nervous system. J Neurosci Res 1994;37:515–528.
Iacobuzio-Donahue CA, Klimstra DS, Adsay NV, Wilentz RE, Argani P, Sohn TA, Yeo CJ, Cameron JL, Kern SE, Hruban RH. Dpc-4 protein is expressed in virtually all human intraductal papillary mucinous neoplasms of the pancreas: comparison with conventional ductal adenocarcinomas. Am J Pathol 2000;157:755–761.
Adsay NV, Conlon KC, Zee SY, Brennan MF, Klimstra DS. Intraductal papillary-mucinous neoplasms of the pancreas: an analysis of in situ and invasive carcinomas in 28 patients. Cancer 2002;94:62–77.
Seidel G, Zahurak M, Iacobuzio-Donahue C, Sohn TA, Adsay NV, Yeo CJ, Lillemoe KD, Cameron JL, Hruban RH, Wilentz RE. Almost all infiltrating colloid carcinomas of the pancreas and periampullary region arise from in situ papillary neoplasms: a study of 39 cases. Am J Surg Pathol 2002;26:56–63.
Maker AV, Lee LS, Raut CP, Clancy TE, Swanson RS. Cytology from pancreatic cysts has marginal utility in surgical decision-making. Ann Surg Oncol 2008;15:3187–3192.
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussant
Dr. Edward Whang (BWU, Boston): Congratulations for a nice study, and congratulations on picking an excellent mentor with whom to work.
I have some tough questions, but I am sure you will be able to handle them.
First, some methodology questions: How did you pick the cases for inclusion in the study? Surely this is a very small subset of IPMNs available to study at MGH.
Also, I noticed the results you presented today are somewhat different from what you wrote in the abstract. In the abstract, you wrote that one of the colloid carcinomas expressed Plectin-1, whereas today, you said four of them expressed Plectin-1. Is there difficulty in interpretation of the immunohistochemistry in the examples that account for that difference?
Now for some philosophical questions: The sensitivity and specificity associated with using Plectin-1 expression status as a basis for distinguishing benign and malignant IPMNs are each less than 85%. Are those performance characteristics sufficient for clinical application?
Lastly, why is it important to differentiate benign from malignant IPMNs preoperatively? Is not the goal of surgery to prevent cancer from developing? Maybe what you really should seek is a biomarker that differentiates benign IPMNs that are destined to become cancer from benign IPMNs that are destined to remain benign for the remainder of the patient’s life.
Closing Discussant
Dr. Dirk Bausch: Invasive carcinoma arising in IPMN is a rare occurrence. Therefore, only a limited number of cases were available to us and included in the study. Benign IPMN and noninvasive malignant IPMN are much more common. For the purpose of the study, an equal number of main duct and branch duct IPMN were assayed. The relatively small number of benign cases compared to malignant cases assayed is a limitation of the study.
Colloid carcinoma cells contain a high amount of mucin, replacing most of the cytoplasm where Plectin-1 is normally identified. This made the evaluation of these samples exceedingly difficult. To accommodate for these difficulties, two independent observers evaluated all slides.
Sensitivity and specificity of Plectin-1 to detect malignant IPMN were about 85%. Currently employed screening methodology to detect malignancy in branch duct IPMNs, such as the international consensus criteria, have a sensitivity of only about 30%. Therefore, the clinical use of Plectin-1 as an additional screening modality may improve the sensitivity to detect malignancy in IPMN substantially.
The distinction between benign and malignant IPMN is important in the case of branch duct IPMNs, which have a relatively low risk of malignancy. Here, the risk associated with surgical therapy can outweigh the risk of malignancy, especially in the elderly population with small IPMNs.
However, it is important that a biomarker for IPMN identifies preinvasive carcinoma in situ, i.e., high-grade dysplasia lesions, whose prognosis is excellent after surgical resection. Plectin-1 identified about 80% of these cases.
Discussant
Dr. Joe Hines (UCLA): Let me ask the goal of this would be to take cyst aspirate to determine if it the cyst benign or malignant?
Closing Discussant
Dr. Dirk Bausch: The aim is to determine if a cyst is benign or malignant by assessing Plectin-1 expression in a cyst fluid aspirate. The goal is to exclude the operator dependency cytology suffers from and to substitute or augment it with an objective assay for Plectin-1.
Discussant
Dr. Joe Hines (UCLA): But my question is, is Plectin-1 shed into the fluid or does the analysis actually require cells? Because, as you said, the ability to access cytologic aspects for these types of lesion is highly unreliable.
Closing Discussant
Dr. Dirk Bausch: In this study, we used cyst fluids obtained from surgical specimens. Since all cyst fluids were centrifuged before being assayed, they should not contain cells. Therefore, Plectin-1 is most likely shed into the fluid itself. However, Plectin-1 content is very low in cyst fluid. Therefore, enrichment by immunoprecipitation was required prior to detection.
Discussant
Dr. Marc Basson (Michigan State University, East Lansing, MI): Do you think that you would you improve on your sensitivity and specificity if you combined the Plectin-1 reactivity with the other clinical criteria that are already in use. Have you gone back and looked at the numbers? I realize they are small.
Closing Discussant
Dr. Dirk Bausch: No such comparison was made in the current study. Our long-term goal is to improve overall sensitivity and specificity by using Plectin-1 together with clinical criteria.
Rights and permissions
About this article
Cite this article
Bausch, D., Mino-Kenudson, M., Fernández-del Castillo, C. et al. Plectin-1 is a Biomarker of Malignant Pancreatic Intraductal Papillary Mucinous Neoplasms. J Gastrointest Surg 13, 1948–1954 (2009). https://doi.org/10.1007/s11605-009-1001-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-009-1001-9