
Abstract
Background
Zenker’s diverticula (ZD) can be treated by transoral diverticulostomy or open surgery (upper esophageal sphincter myotomy and diverticulectomy or diverticulopexy). The aim of this study was to compare the effectiveness of a minimally invasive (group A) versus a traditional open surgical approach (group B) in the treatment of ZD.
Material and Methods
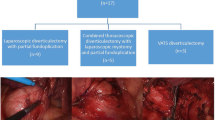
Between 1993 and September 2007, 128 ZD patients underwent transoral diverticulostomy (n = 51) or cricopharyngeal myotomy and diverticulectomy or diverticulopexy (n = 77). All patients were evaluated for symptoms using a detailed questionnaire. Manometry recorded upper esophageal sphincter (UES) pressure, relaxations, and intrabolus pharyngeal pressure. The size of the pouch was measured on the barium swallow. The choice of treatment was based on the size of the diverticulum and the patients’ preference. Long-term follow-up data were available for 121/128 (94.5%) patients with a median follow-up of 40 months (interquartile range, 17–83).
Results
Mortality was nil. Three patients in group A (5.8%) and ten in group B (13%) had postoperative complications (p = n.s.). Hospital stays were markedly shorter for patients after diverticulostomy (p < 0.01). Postoperative manometry showed a reduction in UES pressure, improved UES relaxation, and lower intrabolus pressure in both groups (p < 0.05). Four patients in the open surgery group (5.2%) complained of severe dysphagia after surgery (three of them required endoscopic dilations). In the transoral diverticulostomy group, 11 patients (21.5%) required additional septal reduction (n = 8) or a surgical myotomy (n = 3) for persistent symptoms (p < 0.01); nine of these 11 patients had a ZD ≤ 3 cm in size. After primary and complementary treatments, symptoms disappeared or improved significantly at long-term follow-up in 93.5% of patients in group A and 96% of those in group B.
Conclusion
Diverticulostomy is safe, quick, and effective for most patients with medium-sized ZD, but open surgery offers better long-term results as a primary treatment and should be recommended for younger, healthy patients, especially those with small diverticula. Small ZD may represent a formal contraindication to the transoral approach because an excessively short septum prevents a complete division of the sphincter fibers.


Similar content being viewed by others


References
Killian G. The mouth of the esophagus. Laryngoscope 1907;17:421–428.
Zenker FA, von Ziemssen H. Krankheiten des Oesophagus. In: von Ziemsen H (ed) Handbuch der Speciellen Pathologie und Therapie 1874;7(Suppl). Vogel, Leipzig, pp 1–87
Belsey R. Functional disease of the esophagus. J Thorac Cardiovasc Surg. 1966;52:164–188.
Collard JM, Otte IB, Kestens PJ. Endoscopic stapling technique of esophagodiverticulostomy for Zenker’s diverticulum. Ann Thorac Surg 1993;56:573–576.
Cook IJ, Gabb M, Panagopoulos V. Zenker’s diverticulum is a disorder of upper esophageal sphincter opening. Gastroenterology 1992;103:1229–1235.
Dohlman G, Mattson O. The endoscopic operation for hypopharyngeal diverticula. Arch Otolaryngol 1960;71:744–752.
Ellis FH Jr, Schlegal JF, Lynch VP, Payne WS. Cricopharyngeal myotomy for pharyngo-oesophageal diverticula. Ann Surg. 1969;170:340–349. doi:10.1097/00000658-196909010-00004.
Payne WS. The treatment of pharyngoesophageal diverticulum: the simple and the complex. Hepatogastroenterology 1992;39:109–114.
Omote K, Feussner H, Stein HJ, Ungeheuer A, Siewert JR. Endoscopic stapling diverticulostomy for Zenker’s diverticulum. Surg Endosc 1999;13:535–538. doi:10.1007/s004649901031.
Peracchia A, Bonavina L, Narne S, Segalin A, Antoniazzi L, Marotta G. Minimally invasive surgery for Zenker diverticulum: analysis of results in 95 consecutive patients. Arch Surg 1998;133:695–700. doi:10.1001/archsurg.133.7.695.
Bonavina L, Bona D, Abraham M, Saino G, Abate E. Long-term results of endosurgical and open surgical approach for Zenker diverticulum. World J Gastroenterol 2007;13:2586–2589.
Zaninotto G, Narne S, Costantini M, Molena D, Cutrone C, Portale G, et al. Tailored approach to Zenker’s diverticula. Surg Endosc 2003;17:129–133. doi:10.1007/s00464-002-8806-x.
Passaretti S, Zaninotto G, DiMartino N, Leo P, Costantini M, Baldi F. Standards for oesophageal manometry: a position statement from the Gruppo Italiano di Studio per la Motilita’ Apparato Digerente. Dig Liver Dis 2000;32:46–55. doi:10.1016/S1590-8658(00)80044-4.
Ludlow A. A case of obstructed deglutition from a preternatural dilatation of and bag formed in the pharynx. Med Observ Inq Soc Phys 1769;3:85–101.
Zaninotto G, Costantini M, Boccù C, Anselmino M, Parenti A, Guidolin D, et al. Functional and morphological study of the cricopharyngeal muscle in patients with Zenker’s diverticulum. Br J Surg 1996;83:1263–1267. doi:10.1002/bjs.1800830928.
Lerut T, van Raemdonck D, Guelinckx P, Dom R, Geboes K. Zenker’s diverticulum: is a myotomy of the cricopharyngeus useful? How long should it be? Hepatogastroenterology 1992;39:127–131.
Venturi M, Bonavina L, Colombo L, Antoniazzi L, Bruno A, Mussini E, et al. Biochemical markers of upper esophageal sphincter compliance in patients with Zenker’s diverticulum. J Surg Res 1997;70:46–48. doi:10.1006/jsre.1997.5049.
Shaw DW, Cook IJ, Jamieson GG, Gabb M, Simula ME, Dent J. Influence of surgery on deglutitive upper oesophageal sphincter mechanics in Zenker’s diverticulum. Gut 1996;38:806–811. doi:10.1136/gut.38.6.806.
Ishioka S, Felix VN, Sakai P, Melo J, Pinotti HW. Manometric study of the upper esophageal sphincter before and after endoscopic management of Zenker’s diverticulum. Hepatogastroenterology 1995;42:628–632.
Author information
Authors and Affiliations
Corresponding author
Additional information
Tom R. DeMeester, M.D. (Los Angeles, CA, USA): Dr. Rizzetto, I congratulate you on a well constructed manuscript; I enjoyed reading it. Similarly, I enjoyed listening to your excellent presentation on this rather common problem of Zenker’s diverticulum. The pathophysiology of the problem is largely understood at the present time. I appreciate the focus of your study on the therapeutic approach to the problem. Your study population was large, the follow-up long, and the extent of function studies obtained unique. I commend you on getting preoperative motility studies on these patients. It can be very difficult to get patient consent and to perform. You have nicely shown us and, I think for the first time, documented that a 3-cm diverticulum is not well managed with the endoscopic staple technique and leads to a high rate of recurrence.
I have four questions. First, you had two patients in whom you could not get the staple into the hypopharynx and into the diverticulum and had to convert to an open procedure. In the manuscript, you implied that some patients were difficult to do. Can you describe how hard you tried before you convert, and does the cervical spine or the ability of the patient to extend his head effect your decision to do the transoral procedure?
Second, is a motility study necessary in the common care of these patients at the present time?
Third, Dr. Jean-Marie Collard, who introduced the stapling technique, showed that there were some minor symptoms that persisted in the stapled group other than dysphagia and were due to the large common cavity created when you cut the septum between the diverticulum and the esophagus. Was your symptom evaluation careful enough to pick up those subtleties, or how do you explain the difference between his observation and yours?
Lastly, although this transoral approach suggests that it would protect the recurrent laryngeal nerves, we have seen some nerve palsy following the procedure. They were likely due to stretching of the nerve in trying to get the stapler in the hypopharynx. Would you comment on this and have you seen short-term palsies with this approach?
Christian, it was a superb presentation and, as a previous research fellow in our unit, you have given us reason to be very proud of you.
Christian Rizzetto, M.D. (Padova, Italy): Thank you very much for your kind words and comments. There are several issues to consider in deciding whether or not to perform the transoral procedure. The main appeal of this technique is that no incision is needed and the procedure is quick to complete. Zenker’s diverticula frequently affect elderly patients, however, and the transoral procedure has its drawbacks in certain patients, e.g., if they are unable to open their mouth wide or to overextend their neck (in cases of severe kyphosis). In the two cases you mentioned, it was not easy to position the diverticular scope, and we had a mucosal perforation in one case. Basically, if we consider a patient a suitable candidate for the transoral approach, we normally try this procedure, but if we have trouble inserting the diverticular scope, then we usually opt to convert the procedure.
The second question addresses the manometry issue. I would say that this has been extremely important to our understanding of the pathophysiology of Zenker’s diverticulum and is still important in the preoperative diagnostic work-up, especially in the case of small diverticula. Manometry can also play a part in patients experiencing recurrent dysphagia, to help us understand how it can be managed and the intra-bolus pressure adequately reduced.
Your third question refers to Collard’s study. Our symptom questionnaire focused mainly on dysphagia and regurgitation, but other symptoms were assessed even though they did not count in the symptom score. We observed no differences, however, and the two patient groups were equally satisfied, in our experience at least. I think you have raised an intriguing point that warrants a prospective assessment.
Your last question was about laryngeal nerve palsy. We experienced transient palsy in one case and permanent recurrent laryngeal nerve injury in another: Both patients were in the open surgery group. It is hard to say how this might happen using the transoral approach, but—as you said—they were probably due to stretching of the nerve to accommodate the anvil of the stapler in the hypopharynx. I think exposure is the key issue in this type of surgery: The only way to avoid complications is to ensure adequate vision of the hypopharynx, the diverticulum, and the septum between the sac and the esophagus. In our opinion, the stapler should not be inserted and fired if the exposure conditions are less than optimal.
Rights and permissions
About this article
Cite this article
Rizzetto, C., Zaninotto, G., Costantini, M. et al. Zenker’s Diverticula: Feasibility of a Tailored Approach Based on Diverticulum Size. J Gastrointest Surg 12, 2057–2065 (2008). https://doi.org/10.1007/s11605-008-0684-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-008-0684-7