
Abstract
Introduction
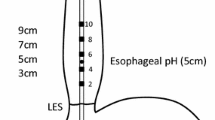
Selecting gastroesophageal reflux disease (GERD) patients for surgery on the basis of standard 24-h pH monitoring may be challenging, particularly if this investigation does not correlate with clinical symptoms. Combined multichannel intraluminal impedance pH monitoring (MII-pH) is able to physically detect each episode of intraesophageal bolus movements, enabling identification of either acid or non-acid reflux episodes and thus establish the association of the reflux with symptoms.
Materials and Methods
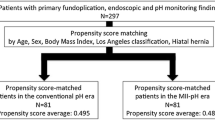
We prospectively assessed and reviewed data from 314 consecutive patients who underwent MII-pH for GERD not responsive or not compliant to proton pump inhibitor therapy. One hundred fifty-three patients with a minimum follow-up of 1 year constituted the study population. Clinical outcomes and satisfaction rate were collected in all patients who underwent laparoscopic Nissen–Rossetti fundoplication. Outcomes were reported for patients with normal and ineffective peristalsis and for patients with positive pH monitoring, negative pH monitoring and positive total number of reflux episodes at MII, and negative pH monitoring and normal number of reflux episodes at MII and a positive symptom index correlation with MII.
Results
The overall patient satisfaction rate was 98.3%. No differences were recorded in the clinical outcomes of the patients with preoperative normal and ineffective peristalsis. No differences in patients’ satisfaction and clinical postoperative DeMeester symptom scoring system were noted between the groups as determined by MII-pH.
Conclusion
MII-pH provides useful information for objective selection of patients to antireflux surgery. Nissen fundoplication provides excellent outcomes in patients with positive and negative pH and positive MII monitoring or Symptom Index association. More extensive studies are needed to definitively standardize the useful MII-pH parameters to select the patient to antireflux surgery.

Similar content being viewed by others

Abbreviations
- GERD:
-
gastroesophageal reflux disease
- MII-pH:
-
combined multichannel intraluminal pH monitoring
- LES:
-
lower esophageal sphincter
- LNRF:
-
laparoscopic Nissen–Rossetti fundoplication
References
Campos GM, Peters JH, DeMeester TR, Oberg S, Crookes PF, Tan S, et al. Multivariate analysis of factors predicting outcome after laparoscopic Nissen fundoplication. J Gastrointest Surg 1999;3:292–300. doi:10.1016/S1091-255X(99)80071-7.
Tutuian R, Castell DO. Review article: complete gastro-oesophageal reflux monitoring—combined pH and impedance. Aliment Pharmacol Ther 2006;24:27–37. doi:10.1111/j.1365-2036.2006.02968.x.
Pizza F, Rosetti G, Del Genio G, Maffettone V, Brusciano L, Del Genio A. Influence of esophageal motility on the outcome of laparoscopic total fundoplication. Dis Esophagus 2008;21:78–85.
Sifrim D, Silny J, Holloway RH, Janssens JJ. Patterns of gas and liquid reflux during transient lower oesophageal sphincter relaxation: a study using intraluminal electrical impedance. Gut 1999;44:47–54.
Sifrim D, Castell D, Dent J, Kahrilas PJ. Gastro-oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut 2004;53:1024–1034. doi:10.1136/gut.2003.033290.
Mainie I, Tutuian R, Agrawal A, Adams D, Castell DO. Combined multichannel intraluminal impedance-pH monitoring to select patients with persistent gastro-oesophageal reflux for laparoscopic Nissen fundoplication. Br J Surg 2006;93:1483–7. doi:10.1002/bjs.5493.
Del Genio G, Rossetti G, Brusciano L, Limongelli P, Pizza F, Tolone S, et al. Laparoscopic Nissen-Rossetti fundoplication with routine use of intraoperative endoscopy and manometry: technical aspects of a standardized technique. World J Surg 2007;31:1099–106. doi:10.1007/s00268-006-0495-5.
del Genio G, Tolone S, Rossetti G, Brusciano L, del Genio F, Pizza F, et al. Total fundoplication does not obstruct the esophageal secondary peristalsis: investigation with pre- and postoperative 24-hour pH-multichannel intraluminal impedance. Eur Surg Res 2008;40:230–234. doi:10.1159/000111146.
Rossetti G, Brusciano L, Amato G, Maffettone V, Napolitano V, Russo G, et al. A total fundoplication is not an obstacle to esophageal emptying after heller myotomy for achalasia: results of a long-term follow up. Ann Surg 2005;241:614–21. doi:10.1097/01.sla.0000157271.69192.96.
Del Genio G, Tolone S, Rossetti G, Brusciano L, Pizza F, del Genio F, et al. Objective assessment of gastroesophageal reflux after extended Heller myotomy and total fundoplication for achalasia with the use of 24 hour combined multichannel intraluminal impedance and pH monitoring (MII-pH). Dis Esophagus 2008, Jun 17 [Epub ahead of print].
Hirano I, Richter JE, Practice Parameters Committee of the American College of Gastroenterology. ACG practice guidelines: Esophageal reflux testing. Am J Gastroenterol 2007;102:668–85. doi:10.1111/j.1572-0241.2006.00936.x.
Vela MF, Camacho-Lobato L, Srinivasan R, Tutuian R, Katz PO, Castell DO. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology 2001;120:1599–606. doi:10.1053/gast.2001.24840.
Tamhankar AP, Peters JH, Portale G, Hsieh CC, Hagen JA, Bremner CG, et al. Omeprazole does not reduce gastroesophageal reflux: new insights using multichannel intraluminal impedance technology. J Gastrointest Surg 2004;8:890–97. doi:10.1016/j.gassur.2004.08.001.
Del Genio G, Tolone S, del Genio F, Rossetti G, Brusciano L, Pizza F, Fei L, del Genio A. The total fundoplication controls acid and non-acid reflux. Evaluation by pre- and postoperative 24 hour pH-multichannel intraluminal impedance. Surg Endosc 2008, May 14. doi:10.1007/s00464-008-9958-0.
Funding/Grant support
None
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
del Genio, G., Tolone, S., del Genio, F. et al. Prospective Assessment of Patient Selection for Antireflux Surgery by Combined Multichannel Intraluminal Impedance pH Monitoring. J Gastrointest Surg 12, 1491–1496 (2008). https://doi.org/10.1007/s11605-008-0583-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-008-0583-y