
Abstract
Background
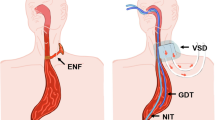
Standard nasogastric decompression following esophagectomy is associated with reduced patient comfort and mobility and impaired hypopharyngeal function—predisposing the patient to sinusitis, pharyngitis, and the risk of aspiration. In this study, we evaluate the results of the transcervical gastric tube drainage in the setting of esophagectomy.
Methods
Transcervical gastric tube decompression was performed on 145 consecutive patients undergoing open esophagectomy between 2003 and 2007. Postoperative outcome variables include morbidity, mortality, esophagostomy duration, and length of stay.
Results
There were 107 males and 38 females (median age = 66; range = 37–87). Perioperative mortality was 2.8%. Major complications included five anastomotic leaks (3.4%), ten pneumonias (6.9%), two myocardial infarctions (1.4%), and the need for reoperation in four patients (bleeding, dehiscence). Median duration of transcervical drainage was 8 days. No tubes were dislodged prematurely. There were no bleeding complications. Four patients developed cellulitis near the cervical gastric tube site and were treated successfully with antibiotics and/or tube removal.
Conclusions
Transcervical gastric decompression can be performed safely with minimal complication risk. Inadvertent tube removal was not encountered in this series. The use of this technique may help to promote accelerated patient mobilization, greater patient comfort, and a durable means of gastric decompression.




Similar content being viewed by others
References
Shackcloth MJ, McCarron E, Kendall J, Russell GN, Pennefather SH, Tran J, Page RD. Randomized clinical trial to determine the effect of nasogastric drainage on tracheal acid aspiration following oesophagectomy. Br J Surg 2006;93(5):547–552.
Lum Cheong RS, Cromwell EE 3rd. Suppurative sinusitis in critically ill patients: a case report and review of the literature. J Natl Med Assoc 1992;84(12):1057–1059.
English G, Morfit H, Ratzer E. Cervical esophagostomy in head and neck cancer. Arch Otolaryngol 1970;92:335.
Royster H, Noone R, Graham W, Theogaraj D. Cervical pharyngostomy for feeding after maxillofacial surgery. Am J Surg 1968;116:610–614.
Graham W, Royster H. Simplified cervical esophagostomy for long-term enteral feeding. Surg Gynecol Obstet 1967;125:127–128.
Singh D, Maley RH, Santucci T, Macherey RS, Bartley S, Weyant RJ, Landreneau RJ. Experience and technique of stapled mechanical cervical esophagogastric anastomosis. Ann Thorac Surg 2001;71:419–424.
Mathisen DJ, Grillo HC, Wilkins EW Jr, Moncure AC, Hilgenburg AD. Transthoracic esophagectomy: a safe approach to carcinoma of the esophagus. Ann Thorac Surg 1988;45(2):137–143.
McKeown KC. The surgical treatment of carcinoma of the oesophagus. A review of the results in 478 cases. J R Coll Surg Edinb 1985;30(1):1–14.
Meehan S, Wood R, Cushieri A. Percutaneous cervical pharyngostomy: a comfortable and convenient alternative to protracted nasogastric intubation. Am J Surg 1984;148:325–330.
Katsoulis I, Livingstone J, Sagor G. Tube pharyngostomy: A simple method for prolonged intubation of the foregut following oesophagogastric surgery. Dig Surg 2006;23:292–295.
Lyons J. Cervical pharyngostomy: a safe alternative for gastrointestinal decompression. Am J Surg 1974;127:387–391.
Patil P, Warad N, Patil R, Kotrashetti S. Cervical pharyngostomy: an alternative approach to enteral feeding. Oral Surg Oral Med Oral Pathol Oral Radiol Endo 2006;102:736–740.
Edge C, Langdon J. Complications of pharyngostomy. Br J Oral Maxillofac Surg 1991;29:237–240.
Hoffmann S, Koller M, Plaul U, Stinner B, Gerdes B, Lorenz W, Rothmund M. Nasogastric tube versus gastrostomy tube for gastric decompression in abdominal surgery: a prospective, randomized trial comparing patients’ tube-related inconvenience. Langenbeck’s Arch Surg 2001;386(6):402–409.
Higaki F, Oishi M, Higaki T, Hayata Y. Old-fashioned but modern tube cervical esophagostomy. Am J Surg 2006;192(3):385–387.
Santos RS, Raftopoulos Y, Singh D, DeHoyos A, Fernando HC, Keenan RJ, Luketich JD, Landreneau RJ. Utility of total mechanical stapled cervical esophagogastric anastomosis after esophagectomy: a comparison to conventional anastomotic techniques. Surgery 2004;136(4):917–925.
Collard JM, Romagnoli R, Goncette L, Otte JB, Kestens PJ. Terminalized semimechanical side-to-side suture technique for cervical esophagogastrostomy. Ann Thorac Surg 1998;65(3):814–817.
Orringer MB, Marshall B, Iannettoni MD. Eliminating the cervical esophagogastric anastomotic leak with a side-to-side stapled anastomosis. J Thorac Cardiovasc Surg 2000;119(2):277–288.
Barros JL. Cervical gastrostomy in the surgical treatment of oesophageal cancer by reconstruction with the stomach. Thorax 1981;36(11):863–865.
Orringer MB, Marshal B, Chang AC, Pickens A, Lau CL. Two thousand transhiatal esophagectomies: changing trends, lessons learned. Ann Surg 2007;246(3):363–372.
Bailey SH, Bull DA, Harpole DH, Rentz JJ, Neumayer LA, Pappas TN, Daley J, Henderson WG, Krasnicka B, Khuri SF. Outcomes after esophagectomy: a ten year prospective cohort. Ann Thorac Surg 2003;75:217–222.
Rizk NP, Bach PB, Schrag D, Bains MS, Turnbull AD, Karpeh M, Brennan MF, Rusch VW. The impact of complications on outcomes after resection for esophageal and gastroesophageal junction carcinoma. J Am Coll Surg 2004;198:42–50.
Portale G, Hagan JA, Peters JH, Chan LS, DeMeester SR, Gandamihardja TA, DeMeester TR. Modern 5-year survival of resectable esophageal adenocarcinoma: single institution experience with 263 patients. J Am Coll Surg 2002;202(4):588–596.
Acknowledgements
The authors wish to acknowledge the important contributions of Kathy Lovas, Theresa Krupka, Diane Sabilla, and Darla Justus in database organization and management.
Author information
Authors and Affiliations
Corresponding author
Additional information
Meeting Presentation: The Society for Surgery of the Alimentary Tract 48th Annual Meeting, Washington D.C., May 19–23, 2007.
Rights and permissions
About this article
Cite this article
Schuchert, M.J., Pettiford, B.L., Landreneau, J.P. et al. Transcervical Gastric Tube Drainage Facilitates Patient Mobility and Reduces the Risk of Pulmonary Complications After Esophagectomy. J Gastrointest Surg 12, 1479–1484 (2008). https://doi.org/10.1007/s11605-008-0541-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-008-0541-8