
Abstract
Introduction
Sigmoid diverticulitis is an infection that resolves with conservative management in 70–85% of patients. Some patients require prolonged hospitalization or surgery during their admission. It has been taught that one should expect clinical improvement within 48 h. In this study, we examined whether basic clinical parameters (the maximum temperature and leukocyte count) of patients would predict improvement and discharge as expected, or prolonged hospitalization.
Materials and Methods
Data was acquired from 198 patients admitted with acute sigmoid diverticulitis as confirmed by computed tomography (CT) scanning and physical exam. One hundred sixty-five patients recovered without surgery with an average hospital stay of 4 days: 120 were discharged within 4 days, whereas 45 patients required longer stays. Nineteen patients underwent surgery early during their admission (within 48 h). Fourteen patients did not improve over time and required surgery later during their hospital stay. The daily maximum temperature and leukocyte count of patients with prolonged stays was compared to the patients who were discharged within 4 days using analysis of variance analysis.
Results
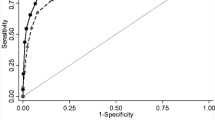
The average maximum temperature and leukocyte count on admission were not statistically different between the groups; therefore, maximum temperature and leukocyte count on admission alone are not predictive. After the first 24 h, however, one could see a statistically significant difference in maximum temperature (p = 0.004). The leukocyte count responded significantly by hospital day 2 (p = 0.003). Both trends were significant through hospital day 4.
Discussion
Patients with a noticeable drop in leukocyte count and maximum temperature over the first 48 h of medical management were predictably discharged early on oral antibiotics. Patients failing to improve at 48 h required prolonged stays or surgery.
Conclusion
By observing early trends in leukocyte count and maximum temperature of patients with diverticulitis, one can predict whether they will recover quickly as expected or if they will likely require prolonged IV antibiotics and/or surgery.

Similar content being viewed by others


References
Parks TG. Natural history of diverticular disease of the colon. A review of 521 cases. Br Med J. 1969;4(5684):639–642.
Smithwick RH. Experience with surgical management of diverticulitis of the sigmoid. Ann Surg 1942;115:969–983.
Boles RS Jr, Jordan S. The clinical significance of diverticulosis. Gastroenterology 1958;35:579–581.
Brown PW, Marcley DM. Prognosis of diverticulitis and diverticulosis of the colon. JAMA 1937;109:1328–1333.
Horner JL. A study of diverticulitis of the colon in office practice. Gastroenterology 1952;21:223–229.
McGowan FJ, Wolff WI. Diverticulitis of sigmoid colon. Gastroenterology 1952;21:119–132.
Pemberton J de J, Black BM, Maino CR. Progress in the surgical management of diverticulitis of the sigmoid colon. Surg Gynecol Obstet 1947;85:523–524.
Waugh JM, Walt AJ. Current trends in the surgical treatment of diverticulitis of the sigmoid colon. Surg Clin North Am 1962;42:1267–1276.
Hiltunen KM, Holehmainen H, Vuorinen T, Maitikainen M. Early water-soluble contrast enema in the diagnosis of acute colonic diverticulitis. Dis Colon Rectum 1986;29:635–638.
Sarin S, Boulous PB. Evaluation of current surgical management of acute inflammatory diverticular disease. Ann R Coll Surg Engl 1991;73:278–282.
Detry R, James J, Kartheuser A, et al. Acute localized diverticulitis: optimum management requires accurate staging. Int J Colorectal Dis 1992;7:38–42.
Larson DM, Masters SS, Spiro HM. Medical and surgical therapy in diverticular disease: a comparative study. Gastroenterology 1976;71:734–737.
Haglund U, Hellberg R, Johnsen C, Hulten L. Complicated diverticular disease of the sigmoid colon: an analysis of short and long term outcome in 392 patients. Ann Chir Gynaecol 1979;68:41–46.
Tyau ES, Prystowsky JB, Joehl RJ, Nahrwold DL. Acute diverticulitis—a complicated problem in the immunocompromised patient. Arch Surg 1991;26:855–858.
Chapman JR, Dozois EJ, Wolff BG, Gullerud RE, Larson DR. Diverticulitis: a progressive disease? Do multiple recurrences predict less favorable outcomes. Ann Surg 2006;243:876–883.
Stabile BE, Arnell TD. Diverticular Disease of the Colon. Current Diagnosis and Treatment in Gastroenterology. 2nd ed. New York: McGraw-Hill; 2003.
Broderick-Villa G, Burchette RJ, Collins JC, Abbas MA, Haigh PI. Hospitalization for Acute Diverticulitis does not mandate routine elective colectomy. Arch Surg 2005;140:576–583.
Chautems RC, Ambrosetti P, Ludwig A, Mermillod B, Morel Ph, Soravia C. Long-term follow-up after first acute episode of sigmoid diverticulitis: Is surgery mandatory. Dis Colon Rectum 2002;34:962–966.
Elliot TB, Yego S, Irvin TT. Five-year audit of the acute complications of diverticular disease. Br J Surg 1997;84:535–539.
Makela J, Vuolio S, Kiviniemi H, Laitinen S. Natural history of diverticular disease: When to operate. Dis Colon Rectum 1998;4:1523–1528.
Ulin AW, Pearce AE, Weinstein SF. Diverticular disease of the colon: surgical perspectives in the past decade. Dis Colon Rectum 1981;24:276–281.
Martinez SA, Cheanvechai V, Alasfar FS, et al. Staged laparoscopic resection for complicated sigmoid diverticulitis. Surg Laparosc Endosc Percutan Tech 1999;9(2):99–105.
Floch CL. Diagnosis and Management of Acute Diverticulitis. J Clin Gastroenterol 2006;40(3):136–144.
Kellum JM, Sugerman HJ, Coppa GF, et al. Randomized prospective comparison of cefoxitin and gentamycin-clndamycin in the treatment of acute colon diverticulitis. Clin Ther 1992;14:376–384.
Morris J, Stellato TA, Haaga JR, Lieberman J. The utility of computed tomography in colonic diverticulitis. Ann Surg 1986;204:128–132.
Mueller MH, Glatzle J, Kasparek MS, et al. Long-term outcome of conservative treatment of patients with diverticulitis of the sigmoid colon. Eur J Gastroenterol Hepatol 2005;17:649–654.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s11605-008-0518-7
Rights and permissions
About this article
Cite this article
Evans, J. Does a 48-Hour Rule Predict Outcomes in Patients with Acute Sigmoid Diverticulitis?. J Gastrointest Surg 12, 577–582 (2008). https://doi.org/10.1007/s11605-007-0405-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-007-0405-7