
Abstract
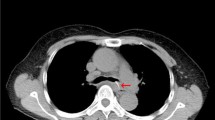
A 68-year-old woman had throat pain while eating fish. The pain gradually disappeared with no treatment. She visited her doctor for a medical checkup 1 year later, and an esophageal tumor was suspected. A double-contrast esophagogram revealed luminal stenosis with a mass-like defect in the middle esophagus. Esophagogastroduodenoscopy (EGD) showed smooth-surface stenosis with a retracted fold. Endoscopic ultrasonography (EUS) showed a hypoechoic mass in the submucosal layer and a well-defined linear hyperechoic structure forming a posterior acoustic shadow within the mass. A computed tomography (CT) examination was then performed using an Aquilion 64-detector row CT scanner, and a high attenuation linear structure was found in the lesion that was visualized as a fish bone-like structure on reconstructed CT images. Endoscopic removal of the fish bone was impossible, and a surgical operation would have been too invasive for a lesion suspected of being benign. The patient had no complaint related to the esophageal lesion itself and no sign of gastrointestinal tract complications. Accordingly, regular follow-up was recommended for the esophageal lesion. Follow-up examination including EGD, esophagography, and CT performed 1 year later showed that the lesion had decreased in size with no fish bone-like structure.
Similar content being viewed by others


References
Watanabe K, Kikuchi T, Katori Y, Fujiwara H, Sugita R, Takasaka T, et al. The usefulness of computed tomography in the diagnosis of impacted fish bones in the oesophagus. J Laryngol Otol 1998;112:360–364.
Al-Qudah A, Daradkeh S, Abu-Khalaf M. Esophageal foreign bodies. Eur J Cardiothorac Surg 1998;13:494–498.
De Lucas EM, Ruiz-Delgado ML, Garcia-Baron PL, Sadaba P, Pagola MA. Foreign esophageal body impaction: multimodality imaging diagnosis. Emerg Radiol 2004;10:216–217.
Ginsberg GG. Management of ingested foreign objects and food bolus impactions. Gastrointest Endosc 1995;41:33–38.
Akazawa Y, Watanabe S, Nobukiyo S, Iwatake H, Seki Y, Umehara T, et al. The management of possible fishbone ingestion. Auris Nasus Larynx 2004;31:413–416.
Ando T, Onda M, Moriyama Y, Tanaka N, Kyono S, Kobayashi T. Three cases of perforation of penetration of digestive tract by ingested fish bone. J Jpn Surg Assoc 1990;23:889–893.
Nanbu K, Sato K, Tamegai Y, Imai S, Uchiyama S, Shibuya T. A case of intraabdominal inflammatory tumor caused by perforation of the transverse colon dueto a fish bone which was preoperatively diagnosed. J Jpn Surg Assoc 1998;59:423–427.
Eliashar R, Dano I, Dangoor E, Braverman I, Sichel JY. Computed tomography diagnosis of esophageal bone impaction: a prospective study. Ann Otol Rhinol Laryngol 1999;108:708–710.
Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, Liao ZA. Endoscopic management of foreign bodies in the upper-GI tract: experience with 1088 cases in China. Gastrointest Endosc 2006;64:485–492.
Kajiura K, Nagamine Y, Kameyama S, Ishimine T, Kohagura F, Fukumoto T. A case of an esophageal foreign body located exclusively in the muscle layer without penetration. J Jpn Surg Assoc 2009;70:1962–1965.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Kikuchi, K., Tsurumaru, D., Hiraka, K. et al. Unusual presentation of an esophageal foreign body granuloma caused by a fish bone: usefulness of multidetector computed tomography. Jpn J Radiol 29, 63–66 (2011). https://doi.org/10.1007/s11604-010-0495-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-010-0495-0