
Abstract
Purpose
This study was performed to validate a highresolution whole-body magnetic resonance angiography (MRA) protocol with parallel imaging and biphasic administration of a single bolus of contrast agent in the preliminary assessment of systemic atherosclerotic burden in patients referred for endovascular procedures.
Materials and methods
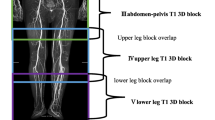
Forty patients referred for endovascular treatment of atherosclerotic disease of the carotid arteries (n=23), peripheral vessels (n=14) or aorta (n=3) on the basis of previous clinical and diagnostic examinations underwent high-resolution whole-body MRA at 1.5 T with 3D spoiled gradient recalled echo (GRE) sequences, featuring parallel imaging acquisition technique with ×2 acceleration factor. Sixty-eight surface coil elements and a four-station imaging protocol were employed. Biphasic intravenous administration of a paramagnetic contrast agent [gadolinium benzyloxyproprionic-tetraacetic acid (Gd-BOPTA)] was performed with the following protocol: 10 ml at a speed of 1 ml/s followed by further 10 ml at a speed of 0.5 ml/s. For image analysis, the arterial system was divided into 42 segments for evaluation. The presence or absence of atherosclerotic lesions was evaluated by two observers in consensus; segments were classified as having clinically significant disease (≥50% stenosis or an aneurysmal dilatation) or no significant disease (<50% stenosis). The presence of stenoocclusive disease, determined at all segments, was compared with findings on digital subtraction angiography (DSA), which were interpreted by a third independent reader. Sensitivity, specificity and concordance of whole-body MRA findings with DSA were calculated, and receiver operating characteristic (ROC) analysis was performed for all vascular territories.
Results
A total of 1,680 arterial segments was evaluated; 138 (8.3%) were affected by atherosclerotic alterations. Carotid lesions were confirmed in 23 patients (34 segments), involvement of peripheral vessels in 14 (57 segments) and abdominal aneurysms in three. Sensitivity and specificity of whole-body MRA were, respectively, 95%–97% for head and neck vessels, 100%-100% for thoracoabdominal vessels, 98%-97% for thigh vessels and 84%–88% for calf vessels; concordance with the DSA findings was significant (p<0.05). Subclinical atherosclerotic lesions were evidenced in 25 patients, involving carotid arteries (12 segments), peripheral vessels (21 segments) and abdominal aorta (one segment). All these lesions were confirmed by a second modality, and ten of these patients required further care.
Conclusions
High-resolution whole-body MRA with Gd-BOPTA may be considered a reliable modality for imaging systemic atherosclerosis in candidates for endovascular procedures. The subclinical detection of the total atherosclerotic burden has potential implications for secondary care in this population.
Riassunto
Obiettivo
Ottimizzare un protocollo angio-RM whole-body (WB) ad alta risoluzione con tecnica di imaging parallelo e somministrazione bifasica di un singolo bolo di mezzo di contrasto (MdC) nello studio della patologia aterosclerotica sistemica ed effettuare una valutazione preliminare del potenziale diagnostico in pazienti candidati a trattamento endovascolare di lesioni arteriose steno-occlusive.
Materiali e metodi
Quaranta pazienti con indicazione al trattamento endovascolare per patologia steno-occlusiva delle arterie carotidi (n=23), del circolo periferico (n=14) o per aneurismi dell’aorta addominale (n=3) sulla base di precedenti indagini clinico-diagnostiche sono stati studiati con un protocollo angio-RM WB ad alta risoluzione con apparecchiatura a 1,5 T e sequenze 3D-spoiled GRE con tecnica di imaging parallelo e fattore di accelerazione ×2, utilizzando un totale di 68 elementi con protocollo a 4 stazioni. Il MdC è stato somministrato con un protocollo di iniezione bifasica a singolo bolo: 10 ml ad una velocità di iniezione di 1 ml/s seguiti da 10 ml alla velocità di 0,5 ml/s di Gd-BOPTA. Per l’analisi delle immagini il circolo arterioso è stato diviso in 42 segmenti. La presenza o l’assenza di patologia aterosclerotica è stata valutata da due osservatori in consenso; i segmenti sono stati classificati come patologici (stenosi ≥50% o dilatazioni aneurismatiche) o non patologici (<50%). I reperti sono stati paragonati con le immagini DSA interpretate da un lettore indipendente. Sono state calcolate sensibilità, specificià e concordanza statistica con la DSA ed è stata effettuata un’fanalisi di tipo ROC per tutti i territori vascolari.
Risultati
Sono stati valutati in totale 1680 segmenti arteriosi; 138 (8,3%) sono risultati patologici. Lesioni carotidee sono state confermate in 23 pazienti (34 segmenti), interessamento del circolo periferico in 14 (57 segmenti) e aneurismi addominali in 3 pazienti. Sensibilità e specificità dell’angio-RM WB sono state rispettivamente 95%–97% per i vasi di testa e collo, 100%-100% per i vasi toraco-addominali, 98%-97% per i vasi femorali e 84%–88% per i vasi di gamba; la concordanza con la DSA è stata significativa (p<0,05). Lesioni aterosclerotiche asintomatiche sono state evidenziate in 25 pazienti, con coinvolgimento delle arterie carotidi (12 segmenti), del circolo periferico (21 segmenti) e dell’aorta addominale (1 segmento): tutte queste lesioni sono state confermate con una seconda metodica ed in 10 di questi pazienti è stato necessario un ulteriore approccio terapeutico.
Conclusioni
L’angio-RM WB con protocollo ad alta risoluzione e Gd-BOPTA può essere considerata una metodica affidabile per la valutazione del carico sistemico di aterosclerosi in pazienti candidati a trattamento endovascolare per patologia arteriosa steno-ostruttiva. La capacità di individuare lesioni asintomatiche ha un potenziale nell’approccio di prevenzione secondaria.
Similar content being viewed by others

References/Bibliografia
Reddy KS, Yusuf S (1998) Emerging epidemic of cardiovascular disease in developing contries. Circulation 97:597–601
Holland AE, Hak PJ, Koudstaaal ML et al (2003) Comparison between measure of atherosclerosis and risk of stroke: the Rotterdam Study. Stroke 34:2367–2373
Ruehm SG, Goyen M, Barkhausen J et al (2001) Rapid magnetic resonance angiography for detection of atherosclerosis. Lancet 357:1086–1091
Goyen M, Quick HH, Debatin JF et al (2002) Whole-body three-dimensional MR angiography with a rolling table platform: initial clinical experience. Radiology 224:270–277
Goyen M, Herborn CU, Kroger K et al (2003) Detection of atherosclerosis: systemic imaging for systemic disease with whole-body three-dimensional MR angiography: initial experience. Radiology 227:277–282
Goyen M, Herborn CU, Kröger K et al (2006) Total-body 3D magnetic resonance angiography influences the management of patients with peripheral arterial occlusive disease. Eur Radiol 16:685–691
Herborn CU, Goyen M, Quick HH et al (2004) Whole-body 3D MR angiography of patients with peripheral arterial occlusive disease. AJR Am J Roentgenol 182:1427–1434
Fenchel M, Requardt M, Tomaschko K et al (2005) Whole-body MR angiography using a novel 32-receiving-channel MR system with surface coil technology: first clinical experience. J Magn Reson Imaging 21:596–603
Napoli A, Catalano C, Anzidei M et al (2007) Imaging the whole-body atherosclerosis: high resolution magnetic resonance angiography using blood-pool agent. Initial clinical experience. Minerva Cardioangiol 55:291–301
Klessen C, Hein PA, Huppertz A et al (2007) First-pass whole-body magnetic resonance angiography (MRA) using the blood-pool contrast medium gadofosveset trisodium: comparison to gadopentetate dimeglumine. Invest Radiol 42:659–664
Kramer H, Morana G (2007) Wholebody magnetic resonance angiography with blood-pool agents. Eur Radiol 17[Suppl 2]:B24–B29
Lin J, Chen B, Wang JH (2006) Diagnosis of systemic arterial diseases with whole-body 3D contrast-enhanced magnetic resonance angiography. Chin Med J 119:1772–1778
Kirchin MA, Pirovano G, Spinazzi A (1998) Gadobenate dimeglumine (Gd-BOPTA). iAn overview. Invest Radiol 33:798–809
Von Kemp K, van den Brande P, Peterson T et al (1997) Screening for concomitant diseases in peripheral vascular patients. Results of a systematic approach. Int Angiol 16:114–122
Hertzer NR, Beven EG, Young JR et al (1984) Coronary artery disease in peripheral vascular patients. A classification of 1,000 coronary angiograms and results of surgical management. Ann Surg 199:223–233
Alexandrova NA, Gibson WC, Norris JW, Maggisano R (1996) Carotid artery stenosis in peripheral vascular disease. J Vasc Surg 23:645–649
Marek J, Mills JL, Harvich J et al (1996) Utility of routine carotid duplex screening in patients who have claudication. J Vasc Surg 24:572–577
Klop RB, Eikelboom BC, Taks AC et al (1991) Screening of the internal carotid arteries in patients with peripheral vascular disease by colourflow duplex scanning. Eur J Vasc Surg 5:41–45
Tode JF (1995) Endarterectomy for asymptomatic carotid artery stenosis. JAMA 274:1505–1507
Barnett HJM, Eliasziw ME, Meldrum HE, Taylor DW (1996) Do the facts and figures warrant a 10-fold increase in the performance of carotid endoarterectomy on asymptomatic patients? Neurology 46:603–608
Lederle FA, Walker JM, Reinke DB (1988) Selective screening for abdominal aortic aneurysms with physical examination and ultrasound. Arch Intern Med 148:1753–1756
Cooley DA, Carmichael MJ (1984) Abdominal aortic aneurysm. Circulation 70:5–6
Salerno TA, Hermandez P, Lynn RB (1981) Abdominal aortic aneurysm in the elderly. Can J Surg 24:71–72
Weinstein MC, Stason WB (1977) Foundations of cost-effectiveness analysis for the health and medical practices. N Engl J Med 296:716–721
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Napoli, A., Anzidei, M., Marincola, B.C. et al. Optimisation of a high-resolution whole-body MR angiography protocol with parallel imaging and biphasic administration of a single bolus of Gd-BOPTA: preliminary experience in the systemic evaluation of atherosclerotic burden in patients referred for endovascular procedures. Radiol med 114, 538–552 (2009). https://doi.org/10.1007/s11547-009-0384-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-009-0384-8