
Abstract
Purpose
It is unknown to what extent overall survival (OS) of organ-confined (T2N0M0) urothelial carcinoma of the urinary bladder (UCUB) patients differs from age- and sex-matched population-based controls, especially when treatment modalities such as radical cystectomy (RC), trimodal therapy (TMT), or radiotherapy (RT) are considered.
Methods
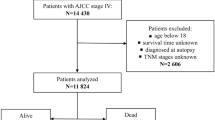
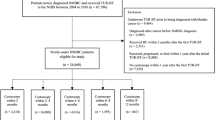
Relying on the Surveillance Epidemiology and End Results database (2004–2018), we identified newly diagnosed (2004–2013) T2N0M0 UCUB patients treated with either RC, TMT or RT. For each case, we simulated an age- and sex-matched control (Monte Carlo simulation), relying on Social Security Administration Life Tables with 5 years of follow-up, and compared OS with that of RC-, TMT-, and RT-treated cases. Additionally, we relied on smoothed cumulative incidence plots to display cancer-specific mortality (CSM) and other-cause mortality (OCM) rates for each treatment modality.
Results
Of 7153 T2N0M0 UCUB patients, 4336 (61%) underwent RC, 1810 (25%) TMT, and 1007 (14%) RT. At 5 years, OS rate in RC cases was 65% vs. 86% in population-based controls (Δ = 21%); in TMT cases, 32% vs. 74% in population-based controls (Δ = 42%); and in RT, 13% vs. 60% in population-based control (Δ = 47%). Five-year CSM rates were highest in RT (57%), followed by TMT (46%) and RC (24%). Five-year OCM rates were the highest in RT (30%), followed by TMT (22%) and RC (12%).
Conclusion
OS of T2N0M0 UCUB patients is substantially less than that of age- and sex-matched population-based controls. The biggest difference affects RT, followed by TMT. A modest difference was recorded in RC and population-based controls.



Similar content being viewed by others

Data availability
All data generated for this analysis were from the Surveillance, Epidemiology, and End Results (SEER) database. The code for the analyses will be made available upon request.
References
J.A. Witjes (Chair), H.M. Bruins, A. Carrión, et al (2022) EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer.
Chang SS, Bochner BH, Chou R et al (2017) Treatment of non-metastatic muscle-invasive bladder cancer: AUA/ASCO/ASTRO/SUO guideline. J Urol 198(3):552–559
Social Security Administration Actuarial Life Table. https://www.ssa.gov/oact/STATS/table4c6.html. Accessed 12 Jul 2022
Howlader N, Noone AM, Krapcho M, et al SEER Cancer Statistics Review, 1975–2018, National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/csr/1975_2018/, based on November 2020 SEER data submission, posted to the SEER web site, April 2021.
Würnschimmel C, Wenzel M, Wang N et al (2021) Long-term overall survival of radical prostatectomy patients is often superior to the general population: a comparison using life-table data. Prostate. https://doi.org/10.1002/pros.24176
Würnschimmel C, Wenzel M, Coll Ruvolo C et al (2021) Life expectancy in metastatic prostate cancer patients according to racial/ethnic groups. Int J Urol 28:862–869. https://doi.org/10.1111/iju.14595
Chierigo F, Borghesi M, Würnschimmel C et al (2022) Life expectancy in metastatic urothelial bladder cancer patients according to race/ethnicity. Int Urol Nephrol. https://doi.org/10.1007/s11255-022-03221-5
Preisser F, Bandini M, Mazzone E et al (2019) Validation of the social security administration life tables (2004–2014) in localized prostate cancer patients within the surveillance, epidemiology, and end results database. Eur Urol Focus 5:807–814. https://doi.org/10.1016/j.euf.2018.05.006
R: The R Project for Statistical Computing. https:// www.r- project. org/. Accessed 12 Jun 2022
Deuker M, Krimphove MJ, Stolzenbach LF et al (2021) Radical cystectomy vs. multimodality treatment in T2N0M0 bladder cancer: a population-based age-matched analysis. Clin Genitourin Cancer 19:e264–e271. https://doi.org/10.1016/j.clgc.2021.03.010
Seisen T, Sun M, Lipsitz SR et al (2017) comparative effectiveness of trimodal therapy versus radical cystectomy for localized muscle-invasive urothelial carcinoma of the bladder. Eur Urol 72:483–487. https://doi.org/10.1016/j.eururo.2017.03.038
Cahn DB, Handorf EA, Ghiraldi EM et al (2017) Contemporary use trends and survival outcomes in patients undergoing radical cystectomy or bladder-preservation therapy for muscle-invasive bladder cancer. Cancer 123:4337–4382. https://doi.org/10.1002/cncr.30900
Zhong J, Switchenko J, Jegadeesh NK et al (2019) Comparison of outcomes in patients with muscle-invasive bladder cancer treated with radical cystectomy versus bladder preservation HHS Public Access. Am J Clin Oncol 42:36–41. https://doi.org/10.1097/COC.0000000000000471
Häggström C, Garmo H, de Luna X et al (2019) Survival after radiotherapy versus radical cystectomy for primary muscle-invasive bladder cancer: a Swedish nationwide population-based cohort study. Cancer Med 8:2196–2204. https://doi.org/10.1002/cam4.2126
Kaushik D, Wang H, Michalek J et al (2019) Chemoradiation versus radical cystectomy for muscle-invasive bladder cancer: a propensity score-weighted comparative analysis using the national cancer database. Urology. https://doi.org/10.1016/j.urology.2019.05.062
Giacalone NJ, Shipley WU, Clayman RH et al (2017) Long-term outcomes after bladder-preserving tri-modality therapy for patients with muscle-invasive bladder cancer: an updated analysis of the massachusetts general hospital experience. Eur Urol 71:952–960. https://doi.org/10.1016/j.eururo.2016.12.020
Würnschimmel C, Wenzel M, Wang N et al (2021) Long-term overall survival of radical prostatectomy patients is often superior to the general population: a comparison using life-table data. Prostate 81:785–793. https://doi.org/10.1002/pros.24176
Acknowledgements
Cristina Cano Garcia was awarded a scholarship by the STIFTUNG GIERSCH.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
Conceptualization: CCG, MLP, PIK; methodology: CCG, ZT, PIK; formal analysis and investigation: CCG, MLP, ST, AP, FB, R-BI; writing—original draft preparation: CCG; writing—review and editing: MLP, ST, AP, FB, R-BI, ZT, FS, AB, CT, SFS, MG, DT, AA, ODeC, MK, SB, LAK, FKHC, PIK; supervision: PIK.
Corresponding author
Ethics declarations
Conflict of interest
Shahrokh F. Shariat: Horonraria: Astellas, Astra Zeneca, Bayer, BMS, Cepheid, Ferring, lpsen, Janssen, Lilly, MSD, Olympus, Pfizer, Pierre Fabre, Richard Wolf, Roche, Sanochemia, Sanofi, Takeda, Urogen. Consulting or Advisory Role: Astellas, Astra Zeneca, Bayer, BMS, Cepheid, Ferring, lpsen, Janssen, Lilly, MSD, Olympus, Pfizer, Pierre Fabre, Richard Wolf, Roche, Sanochemia, Sanofi, Takeda, Urogen. Speakers’ Bureau: Astellas, Astra Zeneca, Bayer, BMS, Cepheid, Ferring, lpsen, Janssen, Lilly, MSD, Olympus, Pfizer, Pierre Fabre, Richard Wolf, Roche, Sanochemia, Sanofi, Takeda, Urogen, Movember Foundation. Patents: Method to determine prognosis after therapy for prostate cancer—granted 2002–09-06, Methods to determine prognosis after therapy for bladder cancer—granted 2003–06-19, Prognostic methods for patients with prostatic disease—granted 2004–08-05; Soluble Fas urinary marker for the detection of bladder transitional cell carcinoma—granted 2010–07-20. Our research was conducted without any other potential conflicts of interest.
Ethical approval
All analyses and their reporting followed the SEER reporting guidelines. Due to the anonymously coded design of the SEER database, study‐specific Institutional Review Board ethics approval was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cano Garcia, C., Piccinelli, M.L., Tappero, S. et al. Differences in overall survival of T2N0M0 bladder cancer patients vs. population-based controls according to treatment modalities. Int Urol Nephrol 55, 1117–1123 (2023). https://doi.org/10.1007/s11255-023-03517-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-023-03517-0