
Abstract
Purpose
Dysmorphic red blood cells (dRBCs) are indicative of glomerular disease and considered a first step in evaluating microscopic hematuria (MH). The predominance of dRBCs does not preclude urological disease; however, some contemporary guidelines advise nephrological evaluation without further urological evaluation, in contrast to the American Urological Association guideline. We investigated the feasibility and safety of omitting urological evaluation in patients presenting with MH.
Methods
A retrospective analysis was performed on 411 consecutive patients who presented with MH between January 2012 and December 2014. MH was defined as ≥3 RBCs per high-power field. All patients received full urological and nephrological evaluations including history and physical assessment, renal function, urine cytology, %dRBC, cystoscopy, computed tomography (CT) imaging, and renal biopsy when indicated.
Results
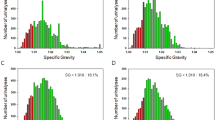
The median %dRBC was higher in patients with glomerular disease than in those with urological disease (40.4 vs. 21.1 %; p < 0.001). Among patients exhibiting %dRBC ≥ 40, 33/97 (34.0 %) had urological and 28/97 (28.9 %) had glomerular diseases. Urological diseases included 9/33 (27.3 %) clinically meaningful malignancies and 17/33 (51.5 %) conditions requiring immediate treatment. The rate of malignancy was comparable between %dRBC groups (p = 0.087). Among patients with final diagnoses who exhibited %dRBC ≥ 40, 32/61 (52.5 %) treatment-requiring conditions would have been unrecognized had cystoscopy and/or CT not been performed. For predicting glomerular disease, the presence of proteinuria demonstrated higher AUC than %dRBC ≥ 40 (0.77 vs. 0.65; p < 0.001).
Conclusions
Identification of %dRBC ≥ 40 had modest diagnostic value in identifying glomerular disease, and concomitant presence of proteinuria was more indicative of glomerular origin in patients presenting with MH. Urological evaluation should not be omitted in these patients considering the prevalence of treatment-requiring urological disease.
Similar content being viewed by others
References
Crop MJ, de Rijke YB, Verhagen PC, Cransberg K, Zietse R (2010) Diagnostic value of urinary dysmorphic erythrocytes in clinical practice. Nephron Clin Pract 115:c203–c212
Buteau A, Seideman CA, Svatek RS, Youssef RF, Chakrabarti G, Reed G et al (2014) What is evaluation of hematuria by primary care physicians? Use of electronic medical records to assess practice patterns with intermediate follow-up. Urol Oncol 32:128–134
Grossfeld GD, Wolf JS Jr, Litwan MS, Hricak H, Shuler CL, Agerter DC et al (2001) Asymptomatic microscopic hematuria in adults: summary of the AUA best practice policy recommendations. Am Fam Physician 63:1145–1154
Fogazzi GB, Edefonti A, Garigali G, Giani M, Zolin A, Raimondi S et al (2008) Urine erythrocyte morphology in patients with microscopic haematuria caused by a glomerulopathy. Pediatr Nephrol 23:1093–1100
Pollock C, Liu PL, Gyory AZ, Grigg R, Gallery ED, Caterson R et al (1989) Dysmorphism of urinary red blood cells–value in diagnosis. Kidney Int 36:1045–1049
Jones R, Latinovic R, Charlton J, Gulliford MC (2007) Alarm symptoms in early diagnosis of cancer in primary care: cohort study using general practice research database. BMJ 334:1040
Niemi MA, Cohen RA (2015) Evaluation of microscopic hematuria: a critical review and proposed algorithm. Adv Chronic Kidney Dis 22:289–296
Davis R, Jones JS, Barocas DA, Castle EP, Lang EK, Leveillee RJ et al (2012) Diagnosis, evaluation and follow-up of asymptomatic microhematuria (AMH) in adults: AUA guideline. J Urol 188:2473–2481
Kiragu D, Cifu AS (2015) Evaluation of patients with asymptomatic microhematuria. JAMA 314:1865–1866
Wollin T, Laroche B, Psooy K (2009) Canadian guidelines for the management of asymptomatic microscopic hematuria in adults. Can Urol Assoc J 3:77–80
Loo R, Whittaker J, Rabrenivich V (2009) National practice recommendations for hematuria: how to evaluate in the absence of strong evidence? Perm J 13:37–46
Roth S, Renner E, Rathert P (1991) Microscopic hematuria: advances in identification of glomerular dysmorphic erythrocytes. J Urol 146:680–684
De Santo NG, Nuzzi F, Capodicasa G, Lama G, Caputo G, Rosati P et al (1987) Phase contrast microscopy of the urine sediment for the diagnosis of glomerular and nonglomerular bleeding-data in children and adults with normal creatinine clearance. Nephron 45:35–39
Nieder AM, Lotan Y, Nuss GR, Langston JP, Vyas S, Manoharan M et al (2010) Are patients with hematuria appropriately referred to Urology? A multi-institutional questionnaire based survey. Urol Oncol 28:500–503
Friedlander DF, Resnick MJ, You C, Bassett J, Yarlagadda V, Penson DF et al (2014) Variation in the intensity of hematuria evaluation: a target for primary care quality improvement. Am J Med 127:633–640
Degrell P, Wagner Z, Szijarto IA, Wagner L, Marko L, Mohas M et al (2008) Morphology of glomerular hematuria is reproduced in vitro by carbonyl stress. Nephron Exp Nephrol 110:e25–e30
Georgopoulos M, Schuster FX, Porpaczy P, Schramek P (1996) Evaluation of asymptomatic microscopic haematuria–influence and clinical relevance of osmolality and pH on urinary erythrocyte morphology. Br J Urol 78:192–196
House AA, Cattran DC (2002) Nephrology: 2. Evaluation of asymptomatic hematuria and proteinuria in adult primary care. CMAJ 166:348–353
Jung H, Gleason JM, Loo RK, Patel HS, Slezak JM, Jacobsen SJ (2011) Association of hematuria on microscopic urinalysis and risk of urinary tract cancer. J Urol 185:1698–1703
El-Galley R, Abo-Kamil R, Burns JR, Phillips J, Kolettis PN (2008) Practical use of investigations in patients with hematuria. J Endourol 22:51–56
Jaffe JS, Ginsberg PC, Gill R, Harkaway RC (2001) A new diagnostic algorithm for the evaluation of microscopic hematuria. Urology 57:889–894
Fairley KF, Birch DF (1982) Hematuria: a simple method for identifying glomerular bleeding. Kidney Int 21:105–108
Mohammad KS, Bdesha AS, Snell ME, Witherow RO, Coleman DV (1993) Phase contrast microscopic examination of urinary erythrocytes to localise source of bleeding: an overlooked technique? J Clin Pathol 46:642–645
Fassett RG, Horgan BA, Mathew TH (1982) Detection of glomerular bleeding by phase-contrast microscopy. Lancet 1:1432–1434
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All of the authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was not required for the purposes of this study as it was based upon retrospective anonymous patient data and did not involve patient intervention or the use of human tissue samples.
Rights and permissions
About this article

Cite this article
Koo, K.C., Lee, K.S., Choi, A.R. et al. Diagnostic impact of dysmorphic red blood cells on evaluating microscopic hematuria: the urologist’s perspective. Int Urol Nephrol 48, 1021–1027 (2016). https://doi.org/10.1007/s11255-016-1265-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1265-4