
Abstract
Objectives
We aimed to compare the success rates of the double hydrodistention implantation technique (HIT) and the HIT with a polyacrylate/polyalcohol copolymer (PPC) for the treatment of primary vesicoureteral reflux (VUR) with a new nonbiodegradable tissue-augmenting substance (Vantris, Promedon, Cordoba, Argentina).
Methods
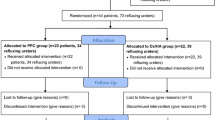
Between January 2011 and December 2012, fifty-two children who underwent subureteric injection for primary VUR are included. The children were randomly separated into two groups, the HIT and the double HIT groups, according to the type of injection. Success was defined as no reflux on a follow-up voiding cystourethrogram (VCUG) after 6 months. The patients were evaluated according to sex, age, grade of reflux, number of injections, and injected volume, and the radiological success rates were compared.
Results
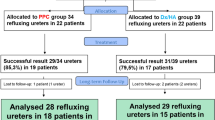
Fifty-two patients underwent an endoscopic injection for primary grade III–V VUR. The HIT group consisted of 26 patients with 33 ureters, and the double HIT group consisted of 26 patients with 35 ureters. There were no significant differences in terms of the sex, ages, VUR grades, bilaterality between the two groups. The mean injected volumes were ml 1.12 (1.02–1.22) in the HIT group and 1.24 ml (95 % CI 1.10–1.38) in the double HIT group. The reflux was resolved in 21/33 (63.6 %) ureters in the HIT group and in 30/35 (85.7 %) ureters in the double HIT group, (p < 0.05). We had only one complication. This patient in the double HIT group, developed bilateral hydronephrosis and oliguric renal failure requiring open reimplantation at the sixth month.
Conclusion
We observed successful results double HIT method with PPC in Grade III–V reflux, but the long-term follow-up of patients is needed for hydronephrosis. As the double HIT treatment leads to a higher success rate, its use is preferable.
Similar content being viewed by others

References
Koyle MA, Elder JS, Skoog SJ, Mattoo TK, Pohl HG, Reddy PP, Abidari JM, Snodgrass WT (2011) Febril urinary tract infection, vesicoureteral reflux, and renal scarring: current controversies in approach to evaluation. Ped Surg Int 27(4):337–346
Khoury A, Bagli D (2007) Reflux and megaureter. In: Wein AJ, Kavoussi LR, Novick AC (eds) Campbell–Walsh urology, chapter 117, 9th edn. WB Saunders, Philadelphia, pp 3423–3481
Ferrer FA, McKenna PH, Hochman HI, Herndon A (1998) Results of a vesicoureteral reflux practice pattern survey among American Academy of Pediatrics, Section on Pediatric Urology members. J Urol 160:1031–1037
O’Donnell B, Puri P (1984) Treatment of vesicoureteric reflux by endoscopic injection of Teflon. Br Med J (Clin Res Ed) 7(289):7–9
Kirsch AJ, Perez-Brayfield M, Smith EA, Scherz HC (2004) The modified sting procedure to correct vesicoureteral reflux: improved results with submucosal implantation within the intramural ureter. J Urol 171:2413–2416
Cerwinka WH, Scherz HC (2008) Kirsch AJ Dynamic hydrodistention classification of the ureter and the double hit method to correct vesicoureteral reflux. Arch Esp Urol 61:882–887
Kalisvaart JF, Scherz HC, Cuda S, Kaye JD, Kirsch AJ (2012) Intermediate to long-term follow-up indicates low risk of recurrence after double HIT endoscopic treatment for primary vesico-ureteral reflux. J Pediatr Urol 8:359–365
Chertin B, Arafeh WA, Kocherov S (2014) Endoscopic correction of complex cases of vesicoureteral reflux utilizing Vantris as a new non-biodegradable tissue-augmenting substance. Pediatr Surg Int 30(4):445–448
Kirsch AJ, Kaye JD, Cerwinka WH, Watson JM, Elmore JM, Lyles RH, Molitierno JA (2009) Scherz HC Dynamic hydrodistention of the ureteral orifice: a novel grading system with high interobserver concordance and correlation with vesicoureteral reflux grade. J Urol 182:1688–1692
Holmdahl G, Brandström P, Läckgren G, Sillén U, Stokland E, Jodal U, Hansson S (2010) The Swedish reflux trial in children: II. Vesicoureteral reflux outcome. J Urol 184:280–285
Matouschek E (1981) Treatment of vesicorenal reflux by transurethral teflon-injection. Urol A 20(5):263–264
Ormaechea M, Ruiz E, Denes E, Gimenez F, Dénes FT, Moldes J, Amarante A, Pioner G, Dekermacher S, de Badiola F (2010) New tissue bulking agent (polyacrylate polyalcohol) for treating vesicoureteral reflux: preliminary results in children. J Urol 183:714–717
Chertin B, Arafeh WA, Zeldin A, Kocherov S (2011) Preliminary data on endoscopic treatment of vesicoureteric reflux with polyacrylate polyalcohol copolymer (Vantris®): surgical outcome following single injection. J Pediatr Urol 7:654–657
Yu TJ (2007) Chang LC The use of collagen for endoscopic correction in complicated vesicoureteral reflux. Scand J Urol Nephrol 41:58–65
Ormaechea M, Paladini M, Pisano R, Scagliotti M, Sambuelli R, Lopez S, Guidi A, Muñoz J, Rossetti V, Carnerero M, Beltramo D, Alasino R, Bianco I, Griguol O, Valladares D, De Badiola F (2008) Vantris: a biocompatible, synthetic, non-biodegradable, easy-to-inject bulking substance. Evaluation of local tissular reaction, localized migration and long-distance migration. Arch Esp Urol 61(2):263–268
Läckgren G, Wåhlin N, Sköldenberg E, Stenberg A (2001) Long-term followup of children treated with dextranomer/hyaluronic acid copolymer for vesicoureteral reflux. J Urol 166:1887–1892
Vandersteen DR, Routh JC, Kirsch AJ, Scherz HC, Ritchey ML, Shapiro E, Wolpert JJ, Pfefferle H (2006) Postoperative ureteral obstruction after suburethral injection of dextranomer/hyaluronic acid copolymer. J Urol 176:1593–1595
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Akin, M., Erginel, B., Karadag, C.A. et al. A comparison of the double hydrodistention implantation technique (HIT) and the HIT with a polyacrylate/polyalcohol copolymer (PPC) for the endoscopic treatment of primary vesicoureteral reflux. Int Urol Nephrol 46, 2057–2061 (2014). https://doi.org/10.1007/s11255-014-0771-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-014-0771-5