
Abstract
Purpose
To the best of our knowledge, no study has compared intermittent steroid pulse therapy, according to Pozzi’s regimen, with versus without tonsillectomy.
Methods
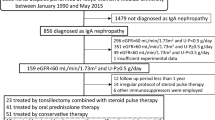
In this retrospective cohort analysis, we compared clinical findings, histological findings according to the Oxford classification, and complete remission rates (RR), defined in terms of urinary protein excretion (U-Prot <0.3 g/g creatinine) and urinary red blood cell count (U-RBC <5/high-power field), after 1 year of treatment in patients with IgA nephropathy (IgAN), who received tonsillectomy with steroid pulse therapy (TSP group, n = 26) or steroid pulse therapy alone (SP group, n = 15).
Results
The baseline clinical and histological characteristics did not differ between the two groups. The RR for U-Prot analyzed by the Kaplan–Meier method did not differ between the groups (76.9 vs. 53.3 %). However, the RR for U-RBC was significantly higher in the TSP than in the SP group (88.4 vs. 33.3 %, log-rank test; P = 0.0008). The RRs for U-Prot and U-RBC were significantly higher in the TSP group than in the SP group (69.2 vs. 13.3 %, log-rank test; P = 0.0019). Cox’s regression analysis showed that combination therapy was associated with higher RR (odds ratio, 12.5; 95 % confidence interval, 2.91–86.7; P = 0.0002).
Conclusions
Tonsillectomy combined with steroid pulse therapy achieved higher RR after 1 year of treatment, compared with steroid pulse monotherapy in patients with IgAN. The long-term effects on renal survival should be analyzed in further studies.




Similar content being viewed by others


References
Berger J, Hinglais N (1968) Inter capillary deposits of IgA-IgG. J Urol Nephrol (Paris) 74:694–695
D’Amico G (2000) Natural history of idiopathic IgA nephropathy: role of clinical and histological prognostic factors. Am J Kidney Dis 36:227–237
Pozzi C, Andrulli S, Del Vecchio L, Melis P, Fogazzi GB, Altieri P, Ponticelli C, Locatelli F (2004) Corticosteroid effectiveness in IgA nephropathy: long-term results of a randomized, controlled trial. J Am Soc Nephrol 15:157–163
Hotta O, Miyazaki M, Furuta T, Tomioka S, Chiba S, Horigome I, Abe K, Taguma Y (2001) Tonsillectomy and steroid pulse therapy significantly impact on clinical remission in patients with IgA nephropathy. Am J Kidney Dis 38:736–743
Komatsu H, Fujimoto S, Hara S, Sato Y, Yamada K, Kitamura K (2008) Effect of tonsillectomy plus steroid pulse therapy on clinical remission of IgA nephropathy: a controlled study. Clin J Am Soc Nephrol 3:1301–1307
A Working Group of the International IgA Nephropathy Network and the Renal Pathology Society (2009) The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Kidney Int 76:534–545
A Working Group of the International IgA Nephropathy Network and the Renal Pathology Society (2009) The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int 76:546–556
Ieiri N, Hotta O, Sato T, Taguma Y (2012) Significance of the duration of nephropathy for achieving clinical remission in patients with IgA nephropathy treated by tonsillectomy and steroid pulse therapy. Clin Exp Nephrol 16:122–129
Pozzi C, Andrulli S, Pani A, Scaini P, Del Vecchio L, Fogazzi G, Vogt B, De Cristofaro V, Allegri L, Cirami L, DeniProcaccini A, Locatelli L (2010) Addition of azathioprine to corticosteroids does not benefit patients with IgA nephropathy. J Am Soc Nephrol 21:1783–1790
Le W, Liang S, Hu Y, Deng K, Bao H, Zeng C, Liu Z (2012) Long-term renal survival and related risk factors in patients with IgA nephropathy: results from a cohort of 1,155 cases in a Chinese adult population. Nephrol Dial Transplant 27:1479–1485
Li PK, Ho KK, Szeto CC, Yu LM, Lai FM (2002) Prognostic indicators of IgA nephropathy in the Chinese—clinical and pathological perspectives. Nephrol Dial Transplant 17:64–69
Sato M, Hotta O, Tomioka S, Horigome I, Chiba S, Miyazaki M, Noshiro H, Taguma Y (2003) Cohort study of advanced IgA nephropathy: efficacy and limitations of corticosteroids with tonsillectomy. Nephron Clin Pract 93:c137–c145
Szeto CC, Lai FM, To KF, Wong TY, Chow KM, Choi PC, Lui SF, Li PK (2001) The natural history of immunoglobulin a nephropathy among patients with hematuria and minimal proteinuria. Am J Med 110:434–437
Shen P, He L, Li Y, Wang Y, Chan M (2007) Natural history and prognostic factors of IgA nephropathy presented with isolated microscopic hematuria in Chinese patients. Nephron Clin Pract 106:c157–c161
Kim BS, Kim YK, Shin YS, Kim YO, Song HC, Kim YS, Choi EJ (2009) Natural history and renal pathology in patients with isolated microscopic hematuria. Korean J Int Med 24:356–361
Manno C, Strippoli GF, D’Altri C, Torres D, Rossini M, Schena FP (2007) A novel simpler histological classification for renal survival in IgA nephropathy: a retrospective study. Am J Kidney Dis 49:763–775
Rauta V, Finne P, Fagerudd J, Rosenlof K, Tornroth T, Gronhagen-Riska C (2002) Factors associated with progression of IgA nephropathy are related to renal function—a model for estimating risk of progression in mild disease. Clin Nephrol 58:85–94
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ochi, A., Moriyama, T., Takei, T. et al. Comparison between steroid pulse therapy alone and in combination with tonsillectomy for IgA nephropathy. Int Urol Nephrol 45, 469–476 (2013). https://doi.org/10.1007/s11255-012-0251-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-012-0251-8