
Abstract
Introduction
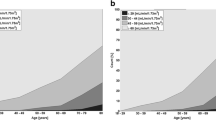
The prevalence of chronic kidney disease (CKD) stages 3 to 5, defined as eGFR <60 ml/min/1.73 m2 for more than three months, in the United Kingdom (UK) is 8%. We investigated the incidence of low eGFR and proteinuria in patients attending our large tertiary referral lipid clinic in 2008.
Methods
In 2008, 1,283 patients were seen, of which 1,029 had complete serum lipid and renal profiles. Estimated glomerular filtration rate (eGFR) was calculated for these patients using the 4-variable MDRD formula. The prevalence of low eGFR (eGFR < 60 ml/min/1.73 m2) and proteinuria (albumin/creatinine ratio >2.4 mg/mmol or urinary protein excretion >0.06 g/l) was calculated.
Results
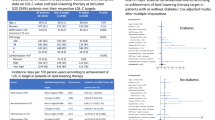
The prevalence of low eGFR and proteinuria was 11.2 and 19.4%, respectively. The percentage of patients with serum lipid levels within the target range suggested by international guidelines was lower among those with low eGFR and proteinuria than in the entire study population, despite similar proportions being treated with statins across all groups.
Conclusions
The prevalences of low eGFR and proteinuria in a group of 1,029 dyslipidaemic patients attending a large tertiary referral lipid clinic were 11.18 and 19.42%, respectively. These levels are much higher than in the general UK population.
Similar content being viewed by others

References
K/DOQI (2002) Clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39(2 Suppl 1):S1–S266
Coresh J, Selvin E, Stevens LA et al (2007) Prevalence of chronic kidney disease in the United States. JAMA 298(17):2038–2047
National Collaborating Centre for Chronic Conditions (2008) Chronic kidney disease. Early identification and management of chronic kidney disease in adults in primary care and secondary care. National Institute for Health and Clinical Excellence Clinical guideline 73, London, UK
Schaeffner E, Kurth T, Curhan G et al (2003) Cholesterol and the risk of renal dysfunction in apparently healthy men. J Am Soc Nephrol 14(8):2084–2091
Caldicott Committee (1997) Report on the review of patient identifiable information. Department of Health, London UK
National Institute for Health and Clinical Excellence (NICE) (2008) Clinical Guideline 66. Available from: www.nice.org.uk/Guidance/CG66
Levey A, Coresh J, Greene T et al (2007) Expressing the modification of diet in renal disease study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin Chem 53(4):766–772
Blaustein D, Kumar R, Goyzueta J (1995) Isolated proteinuria: diagnosis and evaluation. Prim Care Update Ob Gyns 2(6):204–206
Third Report of the National Cholesterol Education Program (NCEP) (2002) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circ 106: 3143
Samuelsson O, Mulec H, Knight-Gibson C et al (1997) Lipoprotein abnormalities are associated with increased rate of progression of human chronic renal insufficiency. Nephrol Dial Transplant 12(9):1908–1915
Muntner P, Coresh J, Smith J et al (2000) Plasma lipids and risk of developing renal dysfunction: the atherosclerosis risk in communities study. Kidney Int 58(1):293–301
Fox C, Larson M, Leip E et al (2004) Predictors of new-onset kidney disease in a community-based population. JAMA 291(7):844–850
Manttari M, Tiula E, Alikoski T et al (1995) Effects of hypertension and dyslipidemia on the decline in renal function. Hypertension 26(4):670–675
Coresh J (2010) Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet (in press)
Landray M, Baigent C, Leaper C et al (2006) The second United Kingdom heart and renal protection (UK-HARP-II) study: a randomized controlled study of the biochemical safety and efficacy of adding ezetimibe to simvastatin as initial therapy among patients with CKD. Am J Kidney Dis 47(3):385–395
Baigent C, Landry M (2003) Study of heart and renal protection (SHARP). Kidney Int Suppl 84:S207–S210
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davies, J.B., Crook, M.A., Wierzbicki, A.S. et al. The incidence of low eGFR and proteinuria in a large tertiary referral lipid clinic. Int Urol Nephrol 43, 821–825 (2011). https://doi.org/10.1007/s11255-010-9819-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-010-9819-3