
Abstract
The left atrial appendage (LAA) is a major source of thromboembolism, particularly in patients with atrial fibrillation (AF). LAA exclusion has arisen as a method of stroke prophylaxis in high-risk patients who have failed medical management, in whom medical management is contraindicated, and in those undergoing concomitant cardiac surgery. Percutaneous LAA exclusion with devices such as the Watchman has been described extensively in the cardiology literature, but surgical exclusion is less often discussed. Several techniques exist for surgical LAA exclusion, including appendage excision (removal), internal ligation from within the left atrium (LA), and external occlusion without opening the LA. The decision of which surgical technique to employ is dependent upon individual patient characteristics including risk factors, surgical history, and appendage anatomy. This paper discusses patient selection for surgical LAA exclusion and methods of surgical exclusion for the non-cardiac surgery medical practitioner.


Similar content being viewed by others
Change history
07 June 2019
In the original version of the article copyright information of Figure 2 was not included in the figure legend.
References
Blackshear JL, Odell JA (1996) Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg 61:755–759
Holmes DR Jr, Kar S, Price MJ et al (2014) Prospective randomized evaluation of the Watchman left atrial appendage closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol 64:1–12
Hui DS, Lee R (2017) Modified internal ligation of the left atrial appendage. J Thorac Cardiovasc Surg 154:847–848
Lee R, Jivan A, Kruse J et al (2013) Late neurologic events after surgery for atrial fibrillation: rare but relevant. Ann Thorac Surg 95:126–131
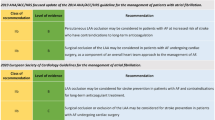
January CT, Wann LS, Alpert JS et al (2014) 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 64:e1–e76
Kirchhof P, Benussi S, Kotecha D et al (2016) 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Kardiol Pol 74:1359–1469
Badhwar V, Rankin JS, Damiano RJ Jr et al (2017) The Society of Thoracic Surgeons 2017 Clinical Practice Guidelines for the Surgical Treatment of Atrial Fibrillation. Ann Thorac Surg 103:329–341
Lee R, Vassallo P, Kruse J et al (2016) A randomized, prospective pilot comparison of 3 atrial appendage elimination techniques: internal ligation, stapled excision, and surgical excision. J Thorac Cardiovasc Surg 152:1075–1080
Hui DS, Abhay LA, Lee R (2015) The Left Atrial Appendage “Lid”: Results of a novel tension-free endocardial exclusion technique. AATS Mitral Conclave, New York
Kanderian AS, Gillinov AM, Pettersson GB et al (2008) Success of surgical left atrial appendage closure: assessment by transesophageal echocardiography. J Am Coll Cardiol 52:924–929
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Greenberg, J.W., Lee, R. & Hui, D.S. Patient selection and methods of surgical left atrial appendage exclusion. J Thromb Thrombolysis 48, 209–214 (2019). https://doi.org/10.1007/s11239-019-01881-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-019-01881-2