
Abstract
Purpose
The aim of this paper is to identify which domains of health-related quality of life (HRQoL) are most important for patients with chronic obstructive pulmonary disease (COPD), from the perspective of healthcare professionals (HCPs).
Methods
Thirteen Dutch HCPs [six pulmonologists, three pulmonology nurse practitioners, two physiotherapists and two general practitioners; 9 men; mean age 51.0 (SD = 10.6) years; mean years of experience 12.1 (SD = 7.2)] specialized in the field of COPD were recruited. The only inclusion criterion was that the HCP had to have extensive experience in treating COPD patients. The face-to-face interviews took 30–40 min.
Results
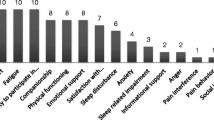
Physical health emerged as the most important theme from the spontaneous statements that HCPs made when asked about HRQoL in relation to COPD, closely followed by social health and coping with COPD-related complaints and restrictions. The most frequently selected PROMIS domains were fatigue, physical function, emotional support and depression. If the related domains satisfaction with participation in social roles and activities and ability to participate in social roles and activities were to be combined, it would come in second place after fatigue.
Conclusion
When comparing the domains chosen by HCPs to the ones chosen by patients in a recent study, there is a high degree of agreement, with the exception of depression. We argue that it is important to take into account both patient and HCP perspective when developing/selecting HRQoL instruments. Our results may be used to inform domain selection to measure HRQoL in patients with COPD, as well as instrument development.

Similar content being viewed by others

References
Lopez, A. D., Shibuya, K., Rao, C., Mathers, C. D., Hansell, A. L., Held, L. S., et al. (2006). Chronic obstructive pulmonary disease: Current burden and future projections. European Respiratory Journal, 27(2), 397–412. doi:10.1183/09031936.06.00025805.
WHO (2013). Chronic obstructive pulmonary disease (COPD) (Fact Sheet No. 315). http://www.who.int/mediacentre/factsheets/fs315/en/. Accessed 13 May 2014.
Nici, L., Donner, C., Wouters, E., Zuwallack, R., Ambrosino, N., Bourbeau, J., et al. (2006). American thoracic society/European respiratory society statement on pulmonary rehabilitation. American Journal of Respiratory and Critical Care Medicine, 173(12), 1390–1413. doi:10.1164/rccm.200508-1211ST.
Global Initiative for Chronic Obstructive Lung Disease. (2007). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management-2007.html.
Pauwels, R. A., Buist, A. S., Calverley, P. M., Jenkins, C. R., & Hurd, S. S. (2001). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO global initiative for chronic obstructive lung disease (GOLD) Workshop summary. American Journal of Respiratory and Critical Care Medicine, 163(5), 1256–1276. doi:10.1164/ajrccm.163.5.2101039.
Velikova, G., Awad, N., Coles-Gale, R., Wright, E. P., Brown, J. M., & Selby, P. J. (2008). The clinical value of quality of life assessment in oncology practice—a qualitative study of patient and physician views. Psycho-Oncology, 17(7), 690–698. doi:10.1002/pon.1295.
Oosterhof, B., Dekker, J. H., Sloots, M., Bartels, E. A., & Dekker, J. (2014). Success or failure of chronic pain rehabilitation: The importance of good interaction—a qualitative study under patients and professionals. Disability and Rehabilitation,. doi:10.3109/09638288.2014.881566.
DiMatteo, M. R. (1998). The role of the physician in the emerging health care environment. Western Journal of Medicine, 168(5), 328–333.
Ha, J. F., & Longnecker, N. (2010). Doctor-patient communication: A review. Ochsner Journal, 10(1), 38–43.
Weldam, S. W., Schuurmans, M. J., Liu, R., & Lammers, J. W. (2012). Evaluation of quality of life instruments for use in COPD care and research: A systematic review. International Journal of Nursing Studies,. doi:10.1016/j.ijnurstu.2012.07.017.
Kruyen, P. M., Emons, W. H. M., & Sijtsma, K. (2013). On the shortcomings of shortened tests: A literature review. International Journal of Testing, 13(3), 223–248. doi:10.1080/15305058.2012.703734.
Kruyen, P. M., Emons, W. H. M., & Sijtsma, K. (2013). Assessing individual change using short tests and questionnaires. Applied Psychological Measurement,. doi:10.1177/0146621613510061.
Paap, M. C. S., Brouwer, D., Glas, C. A. W., Monninkhof, E. M., Forstreuter, B., Pieterse, M. E., et al. (2013). The St George’s respiratory questionnaire revisited: A psychometric evaluation. Quality of Life Research,. doi:10.1007/s11136-013-0570-y.
Barclay-Goddard, R., Epstein, J. D., & Mayo, N. E. (2009). Response shift: A brief overview and proposed research priorities. Quality of Life Research, 18(3), 335–346. doi:10.1007/s11136-009-9450-x.
Ackerman, T. A. (1996). Developments in multidimensional item response theory. Applied Psychological Measurement, 20, 309–310.
Daudey, L., Peters, J. B., Molema, J., Dekhuijzen, P. N., Prins, J. B., Heijdra, Y. F., et al. (2010). Health status in COPD cannot be measured by the St George’s respiratory questionnaire alone: An evaluation of the underlying concepts of this questionnaire. Respiratory Research, 11, 98. doi:10.1186/1465-9921-11-98.
Van der Linden, W. J., & Glas, C. A. W. (Eds.). (2000). Computerized adaptive testing: Theory and practice. Dordrecht: Kluwer.
Embretson, S. E., & Reise, S. (2000). Item response theory for psychologists. Mahwah, NJ: Erlbaum.
Cella, D., Yount, S., Rothrock, N., Gershon, R., Cook, K., Reeve, B., et al. (2007). The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Medical Care, 45(5 Suppl 1), S3–S11. doi:10.1097/01.mlr.0000258615.42478.55.
PROMIS (2014). Domain frameworks PROMIS adult self-reported health. http://www.nihpromis.org/measures/domainframework1. Accessed 25 Feb 2014.
Cella, D., Riley, W., Stone, A., Rothrock, N., Reeve, B., Yount, S., et al. (2010). The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. Journal of Clinical Epidemiology, 63(11), 1179–1194. doi:10.1016/j.jclinepi.2010.04.011.
Fitzsimmons, D., George, S., Payne, S., & Johnson, C. D. (1999). Differences in perception of quality of life issues between health professionals and patients with pancreatic cancer. Psychooncology, 8(2), 135–143.
Brod, M., Tesler, L., & Christensen, T. (2009). Qualitative research and content validity: Developing best practices based on science and experience. Quality of Life Research, 18, 1263–1278.
Terwee, C. B., Roorda, L. D., Vet, H. C. W., Dekker, J., Westhovens, R., Leeuwen, J., et al. (2014). Dutch–Flemish translation of 17 item banks from the Patient-Reported Outcomes Measurement Information System (PROMIS). Quality of Life Research, 1–9, doi:10.1007/s11136-013-0611-6.
Paap, M. C. S., Bode, C., Lenferink, L. I. M., Groen, L. C., Terwee, C. B., Ahmed, S., et al. (2014). Identifying key domains of health-related quality of life for patients with chronic obstructive pulmonary disease: The patient perspective. Health and Quality of Life Outcomes, 12, 106. doi:10.1186/s12955-014-0106-3.
Corbin, J., & Strauss, A. (1990). Grounded theory research: Procedures, canons, and evaluative criteria. Qualitative Sociology, 13(1), 3–21. doi:10.1007/bf00988593.
Victorson, D. E., Anton, S., Hamilton, A., Yount, S., & Cella, D. (2009). A conceptual model of the experience of dyspnea and functional limitations in chronic obstructive pulmonary disease. Value Health, 12(6), 1018–1025. doi:10.1111/j.1524-4733.2009.00547.x.
Bartlett, S. J., Hewlett, S., Bingham, C. O, 3rd, Woodworth, T. G., Alten, R., Pohl, C., et al. (2012). Identifying core domains to assess flare in rheumatoid arthritis: An OMERACT international patient and provider combined Delphi consensus. Annals of the Rheumatic Diseases, 71(11), 1855–1860. doi:10.1136/annrheumdis-2011-201201.
Clark, M., & Hampson, S. E. (2003). Comparison of patients’ and healthcare professionals’ beliefs about and attitudes towards Type 2 diabetes. Diabetic Medicine, 20(2), 152–154. doi:10.1046/j.1464-5491.2003.00896.x.
Woodend, A. K., Nair, R. C., & Tang, A. S. (1997). Definition of life quality from a patient versus health care professional perspective. International Journal of Rehabilitation Research, 20(1), 71–80.
von Leupoldt, A., & Kenn, K. (2013). The psychology of chronic obstructive pulmonary disease. Current Opinion in Psychiatry, 26(5), 458–463. doi:10.1097/YCO.0b013e328363c1fc.
Di Marco, F., Verga, M., Reggente, M., Maria Casanova, F., Santus, P., Blasi, F., et al. (2006). Anxiety and depression in COPD patients: The roles of gender and disease severity. Respiratory Medicine, 100(10), 1767–1774. doi:10.1016/j.rmed.2006.01.026.
Maurer, J., Rebbapragada, V., Borson, S., Goldstein, R., Kunik, M. E., Yohannes, A. M., et al. (2008). Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest, 134(4 Suppl), 43s–56s. doi:10.1378/chest.08-0342.
Zhang, M. W., Ho, R. C., Cheung, M. W., Fu, E., & Mak, A. (2011). Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: A systematic review, meta-analysis and meta-regression. General Hospital Psychiatry, 33(3), 217–223. doi:10.1016/j.genhosppsych.2011.03.009.
Cook, K., Kallen, M., Cella, D., Crane, P., Eldadah, B., Hays, R., et al. (2014). The Patient Reported Outcomes Measurement Information System (PROMIS) Perspective on: Universally-Relevant vs. Disease-Attributed Scales. http://www.nihpromis.org/Universally-Relevant_vs_Disease-Attributed_2014-2-12_final508.pdf. Accessed 11 March 2014.
Acknowledgments
We thank Mitzi Paap, Bachelor of Arts in English language and culture, for translating the interview scheme, tables and quotes from Dutch to English. We also thank all healthcare professionals that participated in this study and Jurrie Eijhuisen for conducting the interviews. This study was supported by Grant #3.4.11.004 from Lung Foundation Netherlands.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix: Script and interview schedule “Interviews with health professionals about quality of life in COPD patients”
Written by Muirne Paap, Christina Bode & Jurrie Eijhuisen, University of Twente
Translated to English by Mitzi Paap
Interviews with health professionals about quality of life in COPD patients
Name interviewer: Jurrie Eijhuisen
Name health professional:
Function health professional:
Date:
Time:
Place:
Introduction
Introducing myself
My name is Jurrie Eijhuisen. I am a private practice physiotherapist. While working as a physiotherapist I study psychology. After completing my bachelor’s degree, I entered a master’s degree in health psychology at the University of Twente, in Enschede. Currently, I am writing my master’s thesis on quality of life in COPD patients from the health professional’s point of view.
Subject
There are all kinds of different questionnaires in existence to assess quality of life in patients with chronic diseases. All these questions can be subdivided into different domains. My research aims to assess, by means of interviews, which of these domains are the most relevant in connection to COPD, according to health professionals. This research study contributes to the development of a computer adaptive test (CAT) which may replace existing paper-and-pencil tests.
Processing data
The interviews will be analyzed and recorded in a report, ensuring anonymity and confidentiality. Possibly, the report will be published as well.
Confidentiality
The research results will be used for scientific purposes only. Your personal information will not be identifiable.
Duration
The interview will take 20–30 minutes
Audio recording
During the interview I will take notes. In addition, I would like to audio record the interview, as it will improve the accuracy of my report. Please, be assured that the audio recordings will be deleted when the research has been completed.
Do you object to the use of an audio recorder during the interview? YES/NO
Any questions or remarks at this stage?

Before we start, I would like to ask you to carefully read this consent form. I want to be certain that you are well informed of the research study. I want to stress that it is not a contract, and that you may withdraw from the study at any time, without giving reasons. By signing this form, you indicate that you have read the aforementioned information and that you agree to the conditions.
–Present consent form–
Central focus
We shall now start the interview. Remember that there are no right or wrong answers. It is about your personal experience and your personal opinion.
–Start audio recording
General questions
I would like to begin with a few general questions (possibly the questions have already been answered through email):
-
What is your profession?

-
Have you got a specialization? YES/NO. If YES, what is your specialization?
-
How long have you been at your current position?



Domains
Now I will pose a few questions regarding different domains of quality of life in COPD patients:
-
In your opinion, how does COPD affect the patient’s quality of life?

-
Can you indicate what the reasons could be?



I will put down sixteen cards in front of you. On these cards, sixteen domains of quality of life are described, each accompanied by a few examples. I would like you to choose five domains of quality of life which, in your view, are the most affected in COPD patients. Try to focus on the general contents of each domain
–let the respondent select five cards–
You indicate that the following five domains are the most affected by COPD:
–read the texts on the five cards aloud–
Carefully study these cards again. Arrange the cards from least important to most important.
–let the respondent arrange the five cards–
The way you have arranged the cards indicates that you consider the following domains as the most relevant in connection with COPD:
1.
2.
3.
4.
5.
–Per domain–:
Can you indicate why this domain is important in connection with COPD?

–When you are using instruments to measure quality of life in COPD patients, do you have a preference for 1 overall score or for specific domain scores ?

–Can you indicate why you prefer 1 overall score / specific domain scores ?

In a previous research study, the same questions were put to COPD patients. They did not all give the same answers. However, the study showed clear preferences in COPD patients.
The four domains the most frequently selected by COPD patients were:
–show cards with the domains concerned–
‘ability to participate in social roles and activities’
‘instrumental support’
‘fatigue’
‘physical functioning’
-
How does this outcome strike you?

-
You have listed five domains of quality of life which, in your view, are the most affected in COPD patients. If you compare your list with the list of preferences in COPD patients, what are the most significant similarities and differences?

-
Can you elaborate on these similarities and/or differences?




Conclusion
-
Is there anything else you would like to add?

-
This is the end of the interview. Have you got any questions or remarks?

-
How do you feel about this interview?




–stop audio recording–
Rights and permissions
About this article

Cite this article
Paap, M.C.S., Bode, C., Lenferink, L.I.M. et al. Identifying key domains of health-related quality of life for patients with chronic obstructive pulmonary disease: interviews with healthcare professionals. Qual Life Res 24, 1351–1367 (2015). https://doi.org/10.1007/s11136-014-0860-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0860-z